
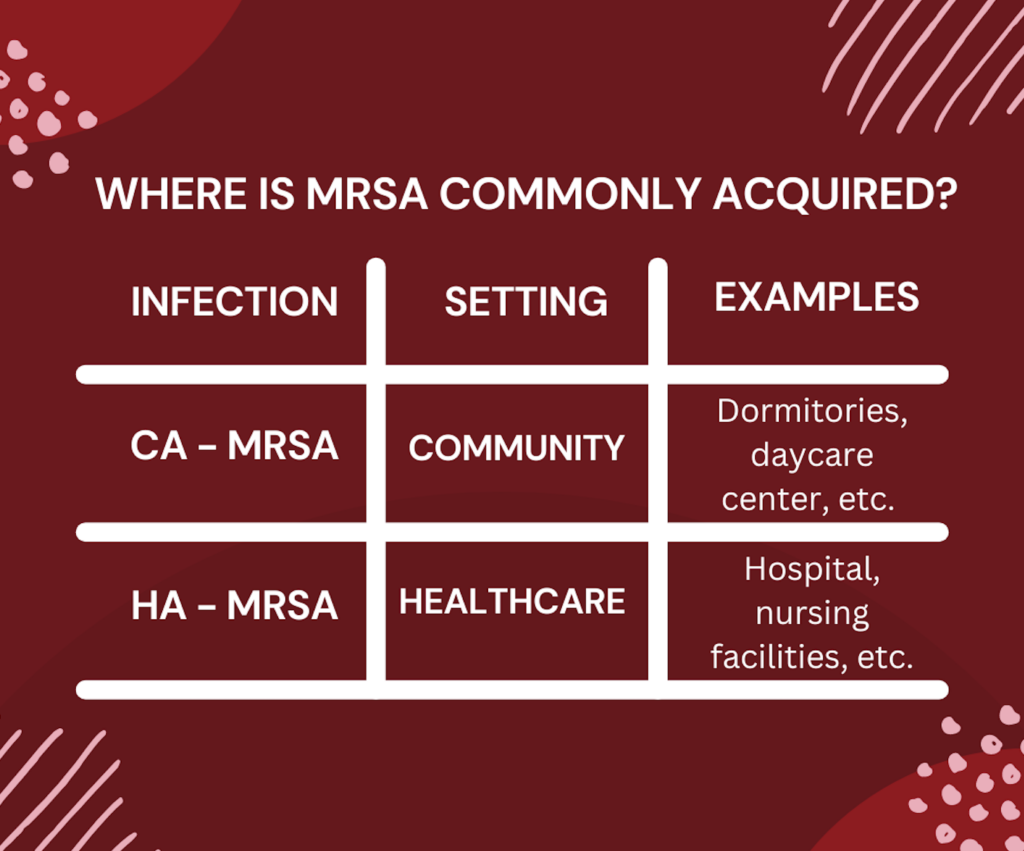
Staphylococcus aureus is a bacteria that can lead to the process of problematic issues in many patients. It is classified and broken down into a few categories, but the main category discussed here will be Methicillin-resistant Staphylococcus aureus (MRSA). MRSA is a type of infection that is hard to treat in clinical settings due to antibiotic resistance. A person can be infected with MSRA in a community setting. This is also known as community-acquired MRSA (CA-MRSA). People may pick up CA-MRSA from workplaces, living environments, or shopping areas. Another setting that a person might get infected with MRSA is in a healthcare setting, also known as hospital-acquired MRSA (HA-MRSA). If MRSA is not treated appropriately, it can lead to serious problems. For this reason, it is important to take all patient-specific factors into account when selecting an antibiotic.
It is important to understand that antibiotic selection is multifactorial, and is also dependent on the site where the bacteria are growing, the patient’s allergies, prior exposure to antibiotics, and their specific susceptibilities. Once susceptibilities come back from the microbiology laboratory and there is confirmation that MRSA is growing from the culture, a decision is made to narrow broad-spectrum antibiotics to other antibiotic agents that specifically target MRSA. In addition, after accessing patient-specific factors, the right antibiotic can be selected that covers these specific bacteria and the duration of therapy can also be determined. Commonly used antibiotics for MRSA infection are:
- Clindamycin
- Vancomycin
- Daptomycin
- Linezolid
- Trimethoprim/sulfamethoxazole
- Doxycycline
- Minocycline
Depending on if patients have CA-MRSA or HA-MRSA, there are different agents that can be started. For example, some antibiotics have only oral options, and some have both intravenous (IV) and oral options. If CA-MRSA is determined, patients are commonly started on oral antibiotics. If HA-MRSA is determined, and patients are in a hospital setting, they will have access to IV antibiotics. Selection of an IV or oral antibiotic and choosing the appropriate dosing is very dependent on the disease state and patient-specific infection factors.
Some antibiotics such as vancomycin need to be monitored. Keeping a watching eye is helpful in determining the right dose for the patient and also if any adjustments are needed to avoid toxicity. The common antibiotic options for the treatment of CA-MRSA are:
- Trimethoprim/sulfamethoxazole,
- Linezolid,
- Doxycycline
- Minocycline
For the treatment of HA-MRSA, the common antibiotic therapies are:
- Vancomycin
- Daptomycin
- Linezolid
- Clindamycin
- Alternative options: Trimethoprim/sulfamethoxazole, doxycycline, and minocycline
The susceptibilities and the area being treated will determine which agent to select because simply choosing an antibiotic that covers MRSA doesn’t necessarily mean it’ll get to the site of action. Also, it is important to determine the right duration for the patient to ensure they have adequate exposure to antibiotics to clear the infection as well as to not expose the patient to unnecessary antibiotic exposure.
Overall, treating infection and picking the correct antibiotic is multifactorial. Some infections are not straightforward and might be difficult to treat even if the correct agent is chosen. It is important to counsel patients on the antibiotic that is started. Patients should complete their antibiotic treatments even if they start to feel better. This is to ensure that the possibility of resistance does not occur. Even though the aforementioned list of MRSA antibiotics are commonly utilized in clinical settings, this is not a comprehensive list available on the market. As with all continuing education, make sure to stay up to date with the current literature, guidelines, and your healthcare-based approaches when treating MRSA infections.
– Dagmara Zajac, RxPharmacist Fall 2022 Intern
References:
- FAQ: The Threat of MRSA: Report on an American Academy of Microbiology Colloquium held in Copenhagen, Denmark, in November 2013. Washington (DC): American Society for Microbiology; 2015. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562897/ doi: 10.1128/AAMCol.Nov.2013
- General information. Centers for Disease Control and Prevention. https://www.cdc.gov/mrsa/community/index.html. Published June 26, 2019. Accessed October 15, 2022.
- Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children [published correction appears in Clin Infect Dis. 2011 Aug 1;53(3):319]. Clin Infect Dis. 2011;52(3):e18-e55. doi:10.1093/cid/ciq146
- MRSA infection. Johns Hopkins Medicine. https://www.hopkinsmedicine.org/health/conditions-and-diseases/mrsa-infection#:~:text=Few%20antibiotics%20are%20available%20to,)%20and%20linezolid%20(Zyvox).>. Accessed October 15, 2022.
- Patel K, Bunachita S, Agarwal AA, Bhamidipati A, Patel UK. A Comprehensive Overview of Antibiotic Selection and the Factors Affecting It. Cureus. 2021;13(3):e13925. Published 2021 Mar 16. doi:10.7759/cureus.13925