A Brief Review on Hypertension for Pharmacists
With so many organ systems, disease states, and medications to remember, preparation for the NAPLEX may often times seem like a daunting task. While there can be a considerable amount of material to go over for each clinical module, there are certainly some things that deserve more focus than others. This brief review will cover some of the most important information you need to know about hypertension when preparing for your upcoming exam.
General information:
- Hypertension (HTN) is asymptomatic
- HTN increases the risk for heart attacks, strokes, and kidney failure
- Risk factors include the following:
- High sodium and fat diet, physical inactivity, obesity, tobacco use, excessive alcohol consumption, genetics and family history, age, sex (women more likely than men), and race (African Americans more likely than any other race)
- Drugs can also increase blood pressure, including the following:
- Amphetamines, cocaine, pseudoephedrine, immunosuppressants, Nonsteroidal anti-inflammatory drugs (NSAIDs), steroids, ethanol, caffeine, serotonin and norepinephrine reuptake inhibitors (SNRIs), oral contraceptives, erythropoietin
Blood pressure categories:

Ultimate blood pressure goal:
- 130/80 mmHg
Treatments:

Four preferred drug classes for the following patient subgroups:
- Non-African American: Thiazide diuretic, CCB, ACE inhibitor or ARB
- African American: Thiazide diuretic
- Patients with chronic kidney disease or diabetes with albuminuria ACE inhibitor or ARB
- Initiate two drugs regimens if blood pressure is > 150/90 mmHg
Additional information:
- ACE inhibitors, ARBs, Aliskiren
- Do not use with Entresto
- Do not use any combination of ACE inhibitors, ARBs, and aliskiren for treatment
- CCBs
- CYP3A4 substrates, avoid CYP3A4 inhibitors (eg, grapefruit)
- Caution with ankle swelling and/or irregular heartbeat
- Amlodipine and felodipine are the safest to use in patients with HF
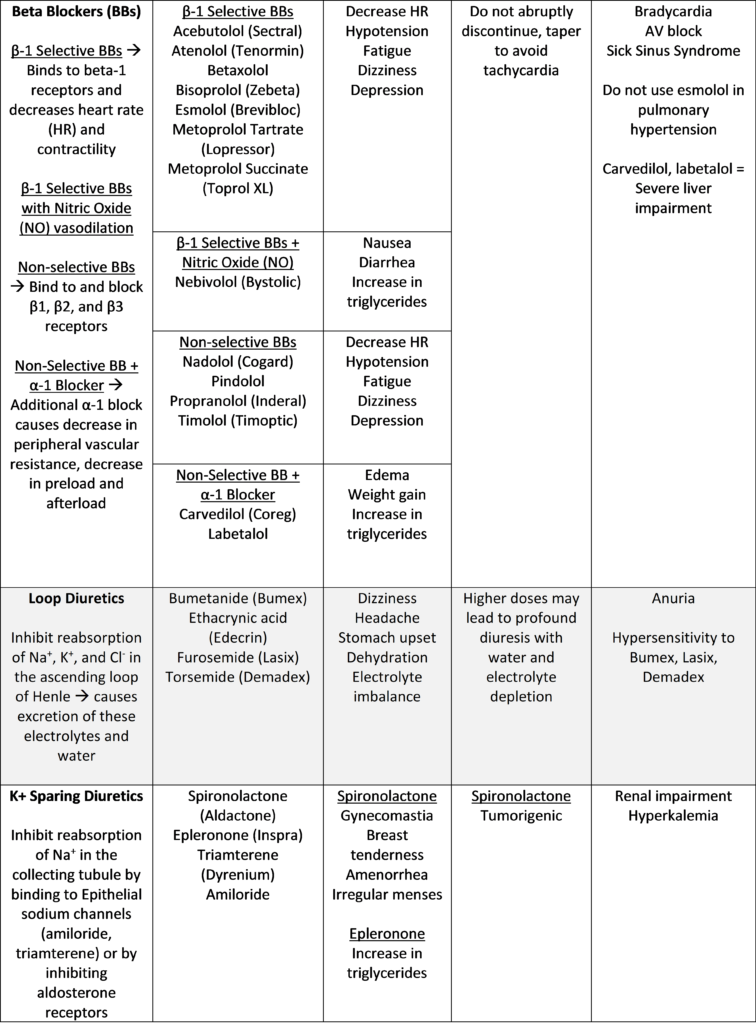
- BBs
- No longer preferred for HTN treatment
- Primarily used first-line for heart disease, post myocardial infarction, and HF
- Use with caution when taking other drugs that decrease HR
- Mask symptoms of hypoglycemia
- No longer preferred for HTN treatment
- Diuretics
- Take doses in the morning or afternoon to avoid frequent urination symptoms at night
- Provide K+ supplementation to compensate for decreased K+ levels
- This does not remain true for K+ sparing diuretics
- Hypertensive emergency
- Blood pressure > 180/120 mmHg
- Acute organ damage
- IV medication used for treatment
- Clevidipine, nicardipine, diltiazem, verapamil, enalaprilat, esmolol, labetalol, metoprolol tartrate, propranolol, nitroglycerin, nitroprusside, chlorothiazide
- Goal is to decrease blood pressure by < 25% within first hour
- Hypertensive urgency
- Blood pressure > 180/20 mmHg
- No organ damages
- Oral medication for treatment
- Pregnancy
- Treatment with labetalol, methyldopa or nifedipine XR
Treatments (non-pharmacological):
- Lifestyle modifications
- DASH diet, limit salt intake (<1,500 mg/day), exercise, limit alcohol consumption, maintain proper weight (BMI between 18.5 – 24.9)
Be on the look-out for our next review, which will focus on diabetes.
Best of luck,
Sam Tamjidi
RxPharmacist Team
References: Micromedex Solutions. Greenwood Village, CO: Truven Health Analytics. http://micromedex.com/. Accessed October 12, 2020.
A Brief Review on Hypertension for Pharmacists Read More »