Residency, Fellowship, post-graduates’ programs; what to choose?
Over the last decade, the profession of pharmacy and the capabilities of a pharmacist has advanced immensely with respect to broader clinical responsibilities and logistical needs in the Pharma industry. We previously lived in a time where a bachelor’s degree in pharmacy sufficed for a career in pharmacy practice. Since 2003; however, the Doctor of Pharmacy (PharmD) degree has superseded previous qualifications to become a licensed pharmacist and has provided pharmacists more holistic roles as a healthcare provider. To dive deeper, the role of a pharmacist now extends from the initial introduction of a chemical molecule for drug therapy all the way to managing a patient’s regimen post dispensing. Based on the competitiveness and saturation of the workforce, in addition to employment projections showing decreased future demand for retail pharmacists (as previously mentioned in our Pharmacist market saturation and career outlook blog here), it is presumed by many that a PharmD will simply be a stepping stone within the realm of pharmacy practice. Therefore, the well-rounded ability needed for our future pharmacists will strongly build through residencies and fellowship.
What are some opportunities to differentiate yourself as a newly graduate? Let’s take a look at the following main categories of post-graduate training programs:
Residencies:
- Focus primarily on direct patient care
- Within a clinical, hospital, or community setting
- Collaborate with pharmacists, nurses, and other healthcare professionals
- Duration: 1 year each – Postgraduate Year One and Two (PGY1 and PGY2)
- PGY1 – General medicine
- PGY2 – Specialized therapeutics
- Specific areas of focus include: Ambulatory care, cardiology, critical care, geriatric, pediatric, oncology, pain management, and more. For a more complete list of options, be sure to check out American Society of Health-System Pharmacists’ (ASHP) website.
- Interestingly enough, the perception of a PGY3 residency has been viewed negatively by many pharmacists. Based on a distributed survey, residents, preceptors, coordinators, and other pharmacists believe that PGY3 training offers limited benefits in professional development.
- Career after completion: Hospital or clinical pharmacist
While clinical and hospital settings are more predominate, many also choose to pursue community-based residency programs. This path allows residents to remain within the community setting while taking on critical education and training to provide increased care and improve patient outcomes.
Another popular residency of interest is managed care. Managed care residencies heavily focus on evidence-based clinical decision-making and comparative research, medication therapy management, clinical drug evaluation, formulary management, quality assurance, and drug utilization review. A pharmacist within these roles is responsible for performing any analysis, for example, drug utilization data to identify trends and then implement new strategies to improve patient outcomes. Additionally these roles may also require on-going knowledge of all heath plan pharmacy benefits. Beyond the logistical aspects of analyses, clinical knowledge is key for a successful career in managed care. Managed care pharmacists are also part of multidisciplinary teams during rounds in which they serve as the primary drug information resource, provide pharmaceutical interventions, facilitate prior authorizations, and develop educational materials for patients and providers.
What’s the likelihood of matching?
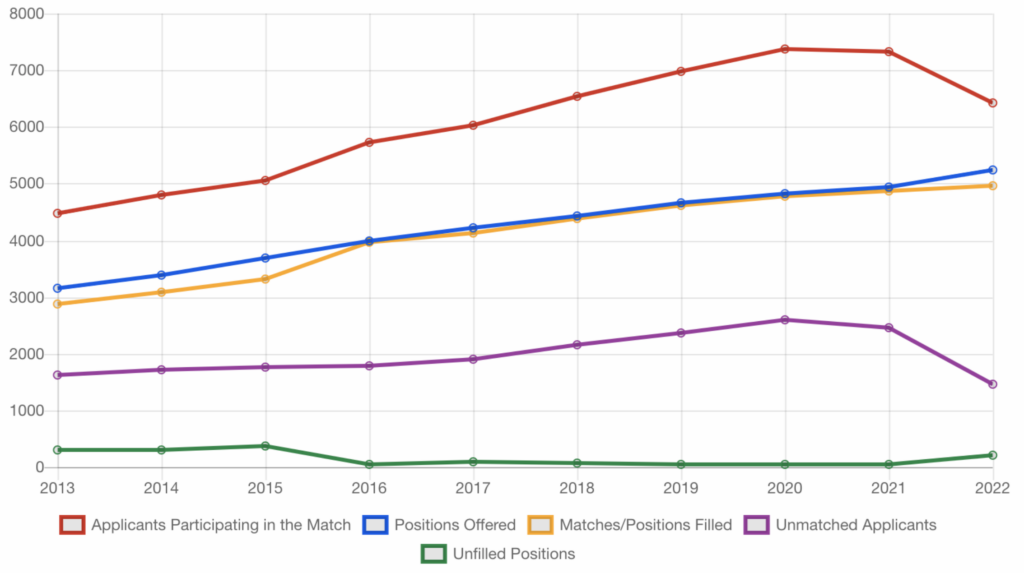
Below is a graphical representation of the match statistics between 2013-2022. Figure 1 illustrates the number of applicants participating in the match, positions offered, matches/positions filled, unmatched applicants, and unfilled positions. Based on the trend, it’s easy to interpret that residency is playing an expanding role as more programs are being introduced each year. There are a few things to note about the trend seen in 2022, specifically the drop in applicants participating in the Match and the decrease in unmatched applicants. Even though this 2022 trend doesn’t have an exact explanation, it is something to watch in future years to understand its direction. Also, there was a rise in 2022 unfilled positions, which has not been seen for a few years and could be indicative of a continued increase in residency programs.
Fellowships:
- More research and data-based
- Within the pharmaceutical industry, academia, nontraditional pharmacy or healthcare setting
- Collaborate with professionals, both in and out of healthcare
- Duration: Ranges between 1-3 years depending on the program
- Career after completion: Pharmaceutical industry or academia
It is very clear that these two main options provide two distinct pathways. The direction you wish to pursue will strictly depend on your interests. If you thoroughly enjoyed classes that focused on therapeutics, pharmacology, and kinetics throughout pharmacy school then a residency may be the best option for you. Conversely, if you were more engaged on the economics, research, and administrative science side of pharmacy, then a fellowship would be better suited for you. Whether you wish to enhance your clinical knowledge or look for professional advancement, a residency or fellowship will provide a firm foundation and present you with many unique career opportunities down the road.
What can you do now and what are some additional resources to find out more?
- Take a moment to fill out the APhA Career Pathway Evaluation Program for Pharmacy Professionals survey. This quiz will aim to assess your goals, values, strengths, likes, and dislikes.
- Maximize your potential and showcase your academic achievements while demonstrating your leadership qualities outside of the classroom.
- Check out the ASHP and ACCP directories to get a better idea of the many residency and fellowship opportunities out there and which institute may best suit you.
Whatever you wish to do is ultimately your decision. Reach out to individuals that took a similar career path that interests you. Ask them questions that will guide you to understand if the career path you are interested in is the right one for you. In today’s world of career networking through social media platforms like LinkedIn, pharmacists can provide you with valuable feedback on why they chose their own journeys and how their choices have impacted their lives over the years. It is crucial to keep seeking advice from other pharmacists who have been where you want to go. Striving for excellence is what we pharmacists know how to do quite well. All we recommend from our end is to be the best version of yourself and manifest all your skills in an effort provide to the pharmacy profession.
Good luck!
Dagmara Zajac
RxPharmacist Team
References:
- Dang, Y. H., To-Lui, K. P. (2020). Pharmacist perceptions of and views on postgraduate year 3 training. American Journal of Health-System Pharmacy, 77(18), 1488-1496. doi:10.1093/ajhp/zxaa198
- Doctor of Pharmacy. (n.d.). Retrieved September 19, 2020, from https://en.wikipedia.org/wiki/Doctor_of_Pharmacy
- Goode, J. R., Owen, J. A., Bennett, M. S., & Burns, A. L. (2019). A marathon, not a sprint: Growth and evolution of community-based pharmacy residency education and training. Journal of the American College of Clinical Pharmacy, 2(4), 402-413. doi:10.1002/jac5.1140
- ASHP Match | Statistics of the Match. Natmatch.com. https://natmatch.com/ashprmp/stats.html. Published 2022. Accessed October 7, 2022.
- Postgraduate Education Frequently Asked Questions: Residencies and Research Fellowships. (n.d.). Retrieved September 17, 2020, from https://www.pharmacist.com/sites/default/files/files/10-417postgraduate.pdf
- Tips on Applying for a Residency or Fellowship. Academy of Managed Care Pharmacy. (n.d.). Retrieved September 19, 2020, from https://www.amcp.org/resource-center/group-resources/residents-fellows/tips-on-applying-residency-fellowship
Residency, Fellowship, post-graduates’ programs; what to choose? Read More »