I recently completed an internship with RxPharmacist, having learned about the opportunity through my school newsletter. I am writing to express my sincere gratitude for the enriching experience and to provide feedback on the valuable insights gained during my time as an intern.
Prior to joining RxPharmacist, I had completed a rotation with a pharmaceutical company in the scientific communications division. It was during this period that I discovered my keen interest in medical writing. Eager to further develop my skills, I applied for the RxPharmacist internship and was thrilled to be accepted.
Throughout my internship, I had the opportunity to work on editing MPJE guides for three different states. Each guide presented a unique set of challenges as they were formatted differently, and the process of understanding and consolidating pharmacy laws from diverse sources proved to be a valuable learning experience. I discovered that not all states provide straightforward access to their laws online. Some require additional effort to compile and update the necessary information for the guides. RxPharmacist MPJE guides combine information from all sources in one document for the purpose of assisting users with simplifying their studying process and ensuring they pass their exams from the first try.
One of the most commendable aspects of the internship was the continuous and detailed feedback I received from my preceptor. Their insights were instrumental in enhancing my medical writing and punctuation skills. I appreciated the accessibility of the preceptors, who could be contacted at any time via Slack and were prompt in responding to queries. The one-on-one sessions offered allowed me to clarify instructions and address any confusion. Interns are fully supported by their preceptors who are always available to answer any questions or confusions.
The feedback received after each project draft proved invaluable, helping me identify and rectify errors I was previously unaware of. I learned various techniques on Microsoft Word to maintain consistent formatting and avoid common pitfalls. I honed my paraphrasing skills while simplifying complex pharmacy laws by properly referencing laws and ensuring accurate representation.
Additionally, the internship provided an opportunity to enhance my question creation skills, a task assigned to generate a specific number of questions for each guide. This not only improved my understanding of the content but also contributed to my preparation for the MPJE exam. Looking at the laws of different states through this internship also raised my awareness on similarities and differences of pharmacist scope of practice in different states which can restrict a pharmacist in one state while permit in another.
Other than the projects, this internship also offers free ‘How to find a job’ live sessions during the fall (as well as for summer internship programs) where students can learn proper resume or CV presentation, how to answer interview questions, how to negotiate salaries, and much more. The instructor is available in the session to ask questions, discuss concerns, and practice elevator pitch and interview questions. This program has helped several students find jobs upon graduation and I am excited to use the skills I learned to find a job once I graduate.
Despite the challenges of managing the internship alongside school commitments during the fall semester, I appreciate the understanding and flexibility demonstrated by my preceptor when extensions were necessary. I wholeheartedly recommend this internship to anyone seeking to improve their medical writing skills.
Thank you once again for the invaluable experience, and I look forward to applying the skills acquired during my time at RxPharmacist in my future endeavors.
The advancement of the pharmacy profession has allowed pharmacists to take on various roles and provide services that extend well beyond what people think. Often times, people think the role of a pharmacist may be assumed as the stereotypical 12-hour workday, consisting of only dispensing medications. However, pharmacists have gone to school for much more than to just dispense, and the magnitude of education and training received throughout school is pertinent to providing exceptional patient care throughout all types of pharmacy. As fellow pharmacists and pharmacy students, we all know too well that we have to go through a rigorous 4-year doctorate program. Pharmacists are now involved with advanced patient-centered services that include transitions of care, medication management, medication reviews with thorough monitoring, chronic disease management, disease education, prevention and wellness services, and patient education. To reinforce how essential they are, pharmacists have been amongst the frontline workers who have played a significant role in reducing the spread of the coronavirus disease 2019 (COVID-19). The extent to which accessibility of a pharmacist in one’s community took national stage when the Department of Health and Human Services (HHS) authorized state-licensed pharmacists to order and administer, and state-licensed or registered pharmacy interns under the supervision of the pharmacist to administer, coronavirus disease 2019 (COVID-19) vaccines to individuals ages 3 or older. Without the efforts of implementing mobile testing facilities, composing response plans, providing curbside delivery, compounding hand sanitizers, and educating the public on methods to prevent spread, the nation’s population may have been much more vulnerable to its virulence. Their highly talented skills, in addition to reasonable accessibility, allows pharmacist to be trusted amongst patients. In fact, pharmacists are rated among the top 5 most trusted professionals year after year by Gallup.
What is provider status?
According to the Social Security Act (SSA), obtaining provider status means pharmacists can participate in Medicare Part B programs and bill Medicare for services under their scope of practice. However, at this time, and despite all their expertise, pharmacists are omitted from this status as the federal government does not consider these health care professionals as medical providers. Currently, those with provider status are professionals employed as physicians, physician’s assistants, certified nurse practitioners, qualified psychologists, clinical social workers, certified nurse midwives, and certified registered nurse anesthetists.
While a large component of this battle surrounds pharmacists fighting to gain provider status under Medicare Part B, reimbursement from Part D also appears to be controversial. Although Medicare Part D reimburses pharmacies for providing medication therapy management to select patients, the program includes only a small set of services that pharmacists are capable of supplying.
What barriers hold pharmacists from reaching this level of authority?
Congress members direct their focus towards the nation’s spending and other issues, including immigration.
Due to financial pressures, those making decisions are more focused on reducing health care expenditure, rather than adding new spending costs.
Congress equates provider status with the “fee-for-service” (FFS) payment model.
FFS is a model in which payment is contingent to the quantity of care, over quality.
Legislators may be unwilling to pursue old payment reform as newer payment models evolve.
Health care professionals with provider status who bill Medicare through the fee-for-service payment model are in a position of strength, both politically and financially.
These individuals may oppose the pharmacy provider status initiative.
While these barriers may impede the ultimate goal of gaining provider status, the American Pharmacist Association (APhA) is taking initiative by contacting health care providers, consumer organizations, payers, and policy makers, all in an effort to educate on the health and economic benefits a pharmacist provides.
What does this mean?
“Provider status is shorthand for ensuring that patients can get access to the clinical services that pharmacists provide and that pharmacists get reimbursed for providing those services” noted vice president of policy for the National Alliance of State Pharmacy Associations, Krystalyn K. Weaver, PharmD. Therefore, this exclusion limits Medicare beneficiaries from accessing pharmacist services.
Tom Menighan, EVP and CEO of APhA, also addressed this concern by stating: “Beyond being unfair to our profession, this lack of federal recognition restricts the contributions pharmacists can make to improving patient care.”
Why is this important?
There is an absolute need to improve health outcomes. In 2016, a released report revealed that the United States spends approximately $1.1 trillion annually on treatment for chronic health conditions, equivalent to almost 6% of the country’s GDP. Additional statistics include the following:
1.5 million cases of preventable medication related side effects
$290 billion spent annually to treat preventable medication related side effects
$100 billion spent annually towards hospitalizations
Improvements in disease state management through proper medication use would not only go a long way in reducing these costs but will also advance patient quality of life in a cost-efficient manner. Who can serve this role and provide comprehensive education to help treat, manage, and prevent diseases? Pharmacists. All evidence through studies and practice-based experience has shown that pharmacists have all the tools to improve health outcomes and reduce health care costs; however, the absence of provider status and proper payment models have obstructed patients and health care providers from accessing full benefits received through pharmacist services. Provided below are opportunities that pharmacists have taken upon to increase health outcomes:
Amidst the ongoing global pandemic we face in today’s world, now is certainly the best time to gain full provider status. As of October 2020, there are only 37 states that have pharmacists classified as “medical providers” under the provisions of Medicare Part B, resulting in a lack of reimbursement for the clinical services provided. Being such an integral part of health care, pharmacists are well-equipped to take on much healthcare challenges, and COVID-19 is reassuring that certainty.
Allow Medicare beneficiaries to access the services provided by a pharmacist
Focus on providing pharmacist care and services to Medicare beneficiaries in medically underserved communities
Provide Medicare reimbursement for pharmacist services in medically underserved communities
The Equitable Community Access to Pharmacist Services Act (H.R. 7213) is also a bipartisan legislation that was introduced in March 2022. This ensures Medicare beneficiary access to pharmacist pandemic-related care without the need for the COVID-19 public health emergency.
Pharmacists have been a vital part of patient care. It is important to recognize healthcare professionals for what they do on an everyday basis. Provider status for pharmacists has been a conversation for a long period of time and with the new legislation in place, the conversation continues. Be a patron, support the cause, because now is the time to reward pharmacists for their purposeful work.
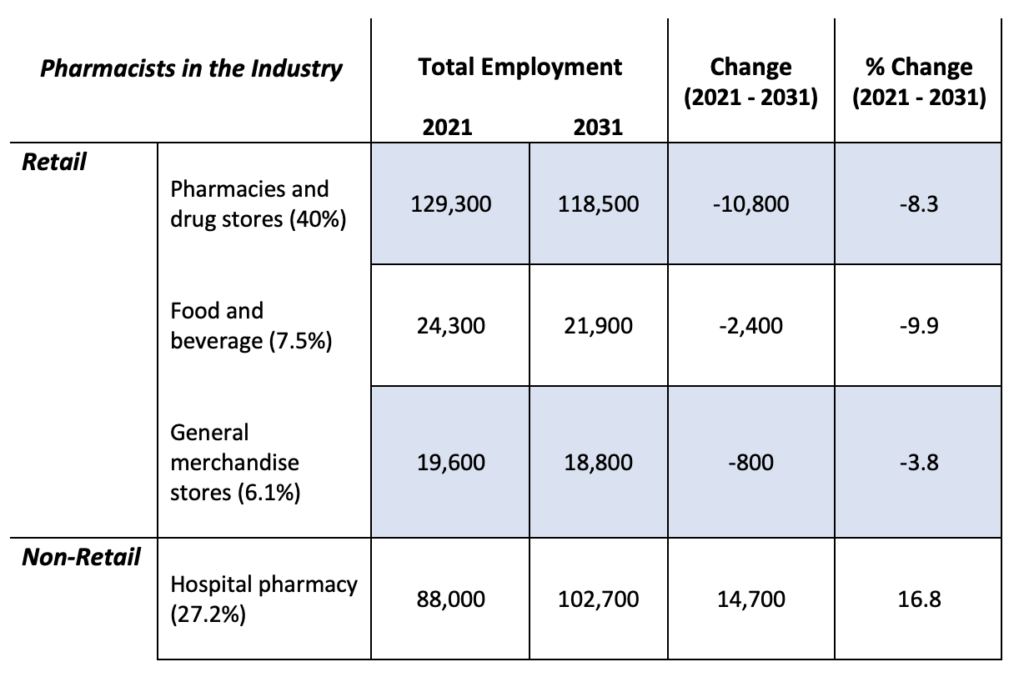
One of the main obstacles that recent PharmD graduates face is the challenge of finding a job right out of school. Whether it is due to saturation or a lack of experience, the dynamic field of pharmacy appears to raise concern for many, and statistics appear to support this concern. According to the U.S. Bureau of Labor Statistics (BLS), which is responsible for publishing employment trends and projections, there is an estimated 2% increase in pharmacist employment between 2021 and 2031. In 2021, there were 323,500 Pharmacist jobs, it is projected by 2031 that number will increase to 331,100 pharmacists jobs. Pharmacist median pay in 2021 was $128,570 per year. While the career outlook of a pharmacist may vary by industry, it is quite evident that most of the decline comes from the chain and independent pharmacies (Table 1).
Table 1. Employment projections for pharmacists in a retail versus non-retail setting.
Table 1 above accounts for 81% (or 261,200 of 323,500) of jobs that pharmacists have held in 2021, while the remaining 19% come from other industries that have a positive effect on the pharmaceutical workforce. A more detailed look at employment projections can be found here.
What can we take home from observing these statistics?
The demand for pharmacists who work in non-retail settings, such as hospitals and ambulatory care facilities, is set to increase over the next decade as the number of jobs are expected to grow. Alternatively, all retail positions, which make up over half of all pharmacy jobs, is projected to take a significant hit and decline over the next 10 years. Why might this be the case? This branch of pharmacy is expected to expand the role of pharmacy technicians and transition to greater use of mail order and online pharmacies. For example, Amazon has expanded its pharmacy by acquiring PillPack and then two years after, it debuted its own Amazon pharmacy. This online service is offered in all 50 states, and it offers most medications except Schedule II controlled substances.
How could you respond and move forward?
Build connections: Use platforms such as LinkedIn to expand your social network and connect and communicate with those in the same profession. Reach out to your school’s alumni network as you already have a shared connection of your alma mater to start off the conversation.
Be comfortable with being uncomfortable: Often you may find more opportunities outside of your city or state of preference. While this may seem unfavorable to begin with, coming out of you comfort zone will always pay off.
Be innovative and embrace change: Demonstrate your passion for excelling the pharmacy profession and show your willingness to flourish. Opportunities will come by with the right mindset.
Overall, pharmacist employment is on the uptrend. Even though some job settings have been seeing downtrends, it’s important to do your research to be well-rounded in knowing what your options are with your pharmacy degree for added job security and flexibility. There are ways to become a competitive individual for the pharmacy job market. It is important to identify areas you want to pursue to know the skills or the experiences you need in order to be a good candidate for your dream job.
It is undeniable that the role of a pharmacist has advanced from the traditional “pill counter” to trusted health care professionals who contribute to patient outcomes through extensive management of drug therapy. According to a published study by the American Association of Colleges of Pharmacy (AACP), the primary practice that PharmD graduates wish to pursue upon graduation is community pharmacy. To outline why this is relevant, the Bureau of Labor Statistics (BLS) anticipates a decline in employment for pharmacists within a traditional retail environment, thus posing a threat to many who wish to follow this route (our full post entitled, “Pharmacist market saturation and career outlook“ can be found here). While all of this may be concerning, pharmacists are fortunately well-equipped with suitable skills that allow them to rise above orthodox practice and pursue nontraditional opportunities while maintaining impactful frontline care. Favorably, the American Society of Health-System Pharmacists (ASHP) has acknowledged this matter and launched its Practice Advancement Initiative (PAI), providing pharmacists with future practice models that may act as an option for those exploring alternative career paths. The campaign advocates for advancing the role of a pharmacist by establishing changes to current pharmacy resources, ultimately promoting career opportunities and patient care simultaneously.
While the number of PharmD graduates continue to increase and advancement of traditional pharmacy begins to slow, you may be asking yourself “what other roles can be filled by pharmacists?” This article will dive into more nontraditional and innovative roles that remain both unique and effective in our dynamic health care world today.
Non-traditional career opportunities:
Type
Description
Where to find information
Nuclear Pharmacy
Nuclear pharmacists focus on the preparation, monitoring, drug information, storage, and handling of radioactive medications. In addition to this, pharmacists in this role provide quality control, patient safety, and counseling to those who require a more unique class of medications. The need for a pharmacist within a nuclear medicine team is impeccable as it allows for a boost in pharmaceutical care to patients.
Specialty medications are typically referred to as high-cost medications that focus more on intricate disease states such as cancer, transplant, hepatitis, HIV, and multiple sclerosis. The prevalence of patients who require specialty medication is increasing, thus necessitating an increased demand for specialty pharmacists who can provide comprehensive care and close management. Due to the increased complexity in the delivery of specialty pharmaceuticals, many health plans have established approaches to help with the obstacles associated with the distribution of these drugs to patients (classified as insourcing and outsourcing):
Insourcing: Staff are hired to manage the high demand and cost of these medications. These pharmacists are responsible for purchasing, handling, educating physicians and patients, and monitoring patient outcomes.
Outsourcing: Contracting with pharmacies that have established specialty pharmaceutical services to access its expertise, technologies, and resources. Regardless of the approach a managed care organization wishes to pursue, both insourcing and outsourcing have identical requirements that include: Negotiating discounted prices, employing staff with specific expertise (with respect to administration, utilization, and monitoring of specialty medications), and accessing centralized distribution points for specialty pharmaceutical manufacturers
While veterinary pharmacy is not a new area of pharmacy practice, it is expected to expand each year and become classified as a more unique career opportunity. Veterinary pharmacists may establish a career with veterinary schools, pharmaceutical companies, manufacturers, and a variety of regulatory agencies (including the FDA through the Center of Veterinary Medicine). An individual interested in working with animals may make this a suitable option; however, additional education and training through residency is required and opportunities are limited usually to academic institutions or professional organizations.
What originally began as physicians taking on both the prescribing and compounding role of patient medication has now evolved to become the responsibility of a pharmacist since the late 19th century. At one point, during the early progression of the 20th century, the manufacturing of mass medications monopolized the service of compounding pharmacies. Today due to the increased need to formulate patient-specific drugs to tailor drug therapy, there appears to be a resurgence in the demand for compounding pharmacists. Compounding services allow pharmacists to prepare medications that target pain management, dermatology, pediatrics, geriatrics, and hormone replacement therapy.
Pharmacists in this role can serve as toxicology specialists within poison control centers. In these centers, they facilitate patients who have ingested or otherwise have been exposed to medications or household chemicals. Pharmacists will direct patients to the proper course of action and will subsequently follow-up with them depending on the severity of the situation.
Telepharmacy aims to meet the needs of today’s healthcare consumers through the use of telecommunication. The application of this tool covers a wide and diverse scope, including drug review and monitoring, dispensing, sterile and non-sterile compounding verification, medication therapy management, patient assessment, patient counseling, clinical consultation, outcomes assessment, decision support, effective drug information, and electronic prescription filling. Telepharmacy technology allows pharmacists to provide communication and remote care delivery. It significantly improves quality of patient care and medication process and safety by increasing accessibility and efficiency through reducing the need to travel. Especially during the ongoing pandemic, telepharmacy has established itself as an attractive tool to positively impact patient outcomes. Individuals who have been tested for COVID-19 could have a consultation with the pharmacist on the phone or video conferencing platforms such as Skype or zoom for follow-up care. Telepharmacy aims to improve U.S. economy and healthcare efficiency.
Pharmacists also play a huge role in regulatory drug and biologic development at the Food and Drug Administration (FDA). Many pharmacists work at the FDA and if you are lucky, you may score a rotation site at the FDA to learn more what they do from drug labels, to drug reviews and ensuring regulations are met.
Pharmacists can pursue consultant pharmacy jobs, such as long-term care pharmacy or home health care pharmacy. This is usually in the setting of hospice, nursing home facilities, group homes, etc. Pharmacists can speak with family members and patients about their treatments. Also, pharmacists can take care of patients with various disease states, such as multiple sclerosis, developmental challenges, etc.
In the industry setting, pharmacists have many opportunities to be involved in. They can strive for research and development, quality assurance, marketing, sales, medical affairs, pharmacovigilance, regulatory affairs, and many other areas. These opportunities can be in the U.S. or global settings. Pharmacists can be involved in many different disease states dependent on the pipeline of a given company.
While additional opportunities may require fellowship or residency training, pharmacists can pursue many different career areas. Doing research on career options can help prepare you early on in your career development in deciding which post-graduation path to prepare for in order to be a great candidate when application season arrives. There are still many other pockets of careers we did not dive into such as hospital pharmacy, medication therapy management (MTM), consulting, and data analytics. The PharmD degree is versatile and allows the flexibility of pharmacists to create their own unique careers outside the ‘box’ of retail and hospital pharmacy. As health care transforms, pharmacy roles will also grow, allowing pharmacists to take on new and unique roles. The American Pharmacist Association (APHA) does a great job of specifically listing many career options for pharmacists, so if you are in a predicament about which career to choose, visit the APHA career option website to learn about the various fields in which pharmacists can utilize their degree.
Bai, S., Hertig, J. B., & Weber, R. J. (2016). Nontraditional Career Opportunities for Pharmacists. Hospital pharmacy, 51(11), 944–949. https://doi.org/10.1310/hpj5111-944
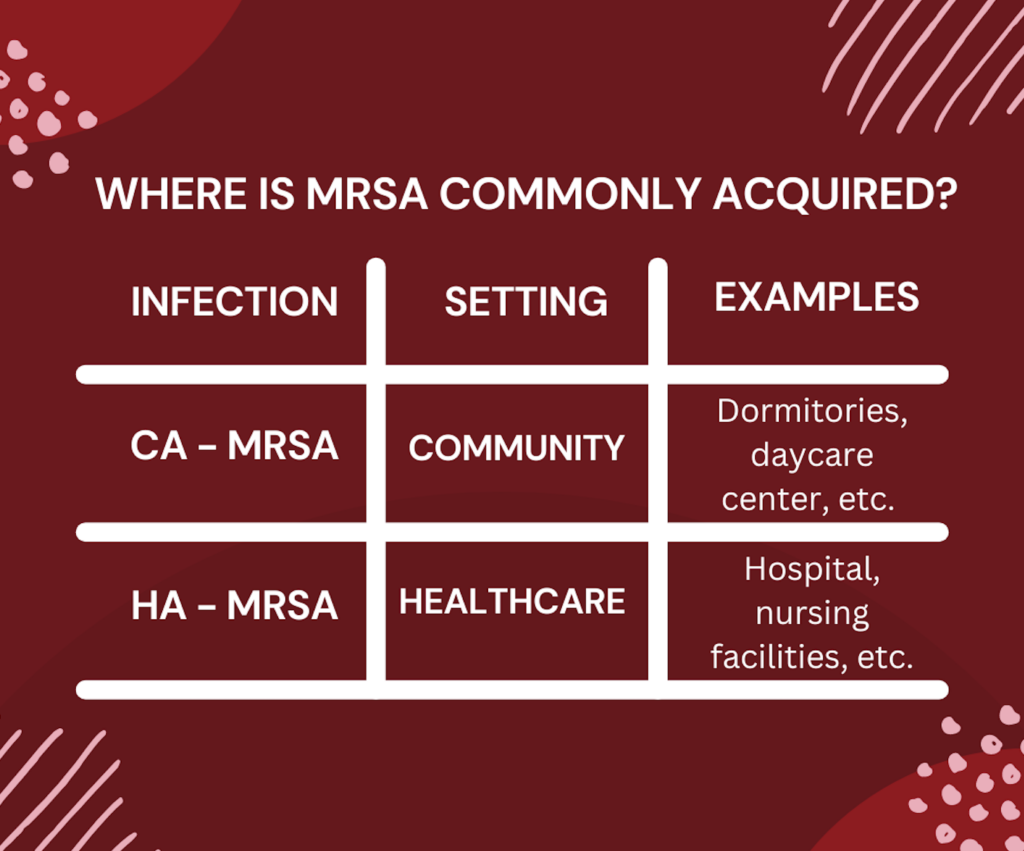
Staphylococcus aureus is a bacteria that can lead to the process of problematic issues in many patients. It is classified and broken down into a few categories, but the main category discussed here will be Methicillin-resistant Staphylococcus aureus (MRSA). MRSA is a type of infection that is hard to treat in clinical settings due to antibiotic resistance. A person can be infected with MSRA in a community setting. This is also known as community-acquired MRSA (CA-MRSA). People may pick up CA-MRSA from workplaces, living environments, or shopping areas. Another setting that a person might get infected with MRSA is in a healthcare setting, also known as hospital-acquired MRSA (HA-MRSA). If MRSA is not treated appropriately, it can lead to serious problems. For this reason, it is important to take all patient-specific factors into account when selecting an antibiotic.
Table: Comparison of CA-MRSA vs. HA-MRSA
It is important to understand that antibiotic selection is multifactorial, and is also dependent on the site where the bacteria are growing, the patient’s allergies, prior exposure to antibiotics, and their specific susceptibilities. Once susceptibilities come back from the microbiology laboratory and there is confirmation that MRSA is growing from the culture, a decision is made to narrow broad-spectrum antibiotics to other antibiotic agents that specifically target MRSA. In addition, after accessing patient-specific factors, the right antibiotic can be selected that covers these specific bacteria and the duration of therapy can also be determined. Commonly used antibiotics for MRSA infection are:
Clindamycin
Vancomycin
Daptomycin
Linezolid
Trimethoprim/sulfamethoxazole
Doxycycline
Minocycline
Depending on if patients have CA-MRSA or HA-MRSA, there are different agents that can be started. For example, some antibiotics have only oral options, and some have both intravenous (IV) and oral options. If CA-MRSA is determined, patients are commonly started on oral antibiotics. If HA-MRSA is determined, and patients are in a hospital setting, they will have access to IV antibiotics. Selection of an IV or oral antibiotic and choosing the appropriate dosing is very dependent on the disease state and patient-specific infection factors.
Some antibiotics such as vancomycin need to be monitored. Keeping a watching eye is helpful in determining the right dose for the patient and also if any adjustments are needed to avoid toxicity. The common antibiotic options for the treatment of CA-MRSA are:
Trimethoprim/sulfamethoxazole,
Linezolid,
Doxycycline
Minocycline
For the treatment of HA-MRSA, the common antibiotic therapies are:
Vancomycin
Daptomycin
Linezolid
Clindamycin
Alternative options: Trimethoprim/sulfamethoxazole, doxycycline, and minocycline
The susceptibilities and the area being treated will determine which agent to select because simply choosing an antibiotic that covers MRSA doesn’t necessarily mean it’ll get to the site of action. Also, it is important to determine the right duration for the patient to ensure they have adequate exposure to antibiotics to clear the infection as well as to not expose the patient to unnecessary antibiotic exposure.
Overall, treating infection and picking the correct antibiotic is multifactorial. Some infections are not straightforward and might be difficult to treat even if the correct agent is chosen. It is important to counsel patients on the antibiotic that is started. Patients should complete their antibiotic treatments even if they start to feel better. This is to ensure that the possibility of resistance does not occur. Even though the aforementioned list of MRSA antibiotics are commonly utilized in clinical settings, this is not a comprehensive list available on the market. As with all continuing education, make sure to stay up to date with the current literature, guidelines, and your healthcare-based approaches when treating MRSA infections.
– Dagmara Zajac, RxPharmacist Fall 2022 Intern
References:
FAQ: The Threat of MRSA: Report on an American Academy of Microbiology Colloquium held in Copenhagen, Denmark, in November 2013. Washington (DC): American Society for Microbiology; 2015. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562897/ doi: 10.1128/AAMCol.Nov.2013
Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children [published correction appears in Clin Infect Dis. 2011 Aug 1;53(3):319]. Clin Infect Dis. 2011;52(3):e18-e55. doi:10.1093/cid/ciq146
Patel K, Bunachita S, Agarwal AA, Bhamidipati A, Patel UK. A Comprehensive Overview of Antibiotic Selection and the Factors Affecting It. Cureus. 2021;13(3):e13925. Published 2021 Mar 16. doi:10.7759/cureus.13925
Over the last decade, the profession of pharmacy and the capabilities of a pharmacist has advanced immensely with respect to broader clinical responsibilities and logistical needs in the Pharma industry. We previously lived in a time where a bachelor’s degree in pharmacy sufficed for a career in pharmacy practice. Since 2003; however, the Doctor of Pharmacy (PharmD) degree has superseded previous qualifications to become a licensed pharmacist and has provided pharmacists more holistic roles as a healthcare provider. To dive deeper, the role of a pharmacist now extends from the initial introduction of a chemical molecule for drug therapy all the way to managing a patient’s regimen post dispensing. Based on the competitiveness and saturation of the workforce, in addition to employment projections showing decreased future demand for retail pharmacists (as previously mentioned in our Pharmacist market saturation and career outlook blog here), it is presumed by many that a PharmD will simply be a stepping stone within the realm of pharmacy practice. Therefore, the well-rounded ability needed for our future pharmacists will strongly build through residencies and fellowship.
What are some opportunities to differentiate yourself as a newly graduate? Let’s take a look at the following main categories of post-graduate training programs:
Residencies:
Focus primarily on direct patient care
Within a clinical, hospital, or community setting
Collaborate with pharmacists, nurses, and other healthcare professionals
Duration: 1 year each – Postgraduate Year One and Two (PGY1 and PGY2)
PGY1 – General medicine
PGY2 – Specialized therapeutics
Specific areas of focus include: Ambulatory care, cardiology, critical care, geriatric, pediatric, oncology, pain management, and more. For a more complete list of options, be sure to check out American Society of Health-System Pharmacists’ (ASHP) website.
Interestingly enough, the perception of a PGY3 residency has been viewed negatively by many pharmacists. Based on a distributed survey, residents, preceptors, coordinators, and other pharmacists believe that PGY3 training offers limited benefits in professional development.
Career after completion: Hospital or clinical pharmacist
While clinical and hospital settings are more predominate, many also choose to pursue community-based residency programs. This path allows residents to remain within the community setting while taking on critical education and training to provide increased care and improve patient outcomes.
Another popular residency of interest is managed care. Managed care residencies heavily focus on evidence-based clinical decision-making and comparative research, medication therapy management, clinical drug evaluation, formulary management, quality assurance, and drug utilization review. A pharmacist within these roles is responsible for performing any analysis, for example, drug utilization data to identify trends and then implement new strategies to improve patient outcomes. Additionally these roles may also require on-going knowledge of all heath plan pharmacy benefits. Beyond the logistical aspects of analyses, clinical knowledge is key for a successful career in managed care. Managed care pharmacists are also part of multidisciplinary teams during rounds in which they serve as the primary drug information resource, provide pharmaceutical interventions, facilitate prior authorizations, and develop educational materials for patients and providers.
What’s the likelihood of matching?
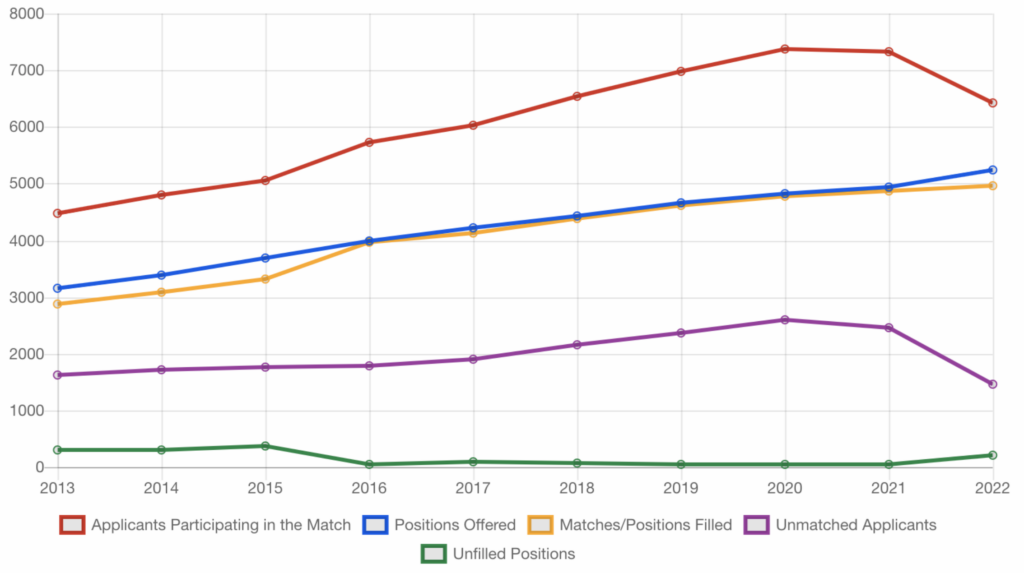
Below is a graphical representation of the match statistics between 2013-2022. Figure 1 illustrates the number of applicants participating in the match, positions offered, matches/positions filled, unmatched applicants, and unfilled positions. Based on the trend, it’s easy to interpret that residency is playing an expanding role as more programs are being introduced each year. There are a few things to note about the trend seen in 2022, specifically the drop in applicants participating in the Match and the decrease in unmatched applicants. Even though this 2022 trend doesn’t have an exact explanation, it is something to watch in future years to understand its direction. Also, there was a rise in 2022 unfilled positions, which has not been seen for a few years and could be indicative of a continued increase in residency programs.
Figure 1. Complete match statistics between 2013-2022.
Fellowships:
More research and data-based
Within the pharmaceutical industry, academia, nontraditional pharmacy or healthcare setting
Collaborate with professionals, both in and out of healthcare
Duration: Ranges between 1-3 years depending on the program
Career after completion: Pharmaceutical industry or academia
It is very clear that these two main options provide two distinct pathways. The direction you wish to pursue will strictly depend on your interests. If you thoroughly enjoyed classes that focused on therapeutics, pharmacology, and kinetics throughout pharmacy school then a residency may be the best option for you. Conversely, if you were more engaged on the economics, research, and administrative science side of pharmacy, then a fellowship would be better suited for you. Whether you wish to enhance your clinical knowledge or look for professional advancement, a residency or fellowship will provide a firm foundation and present you with many unique career opportunities down the road.
What can you do now and what are some additional resources to find out more?
Maximize your potential and showcase your academic achievements while demonstrating your leadership qualities outside of the classroom.
Check out the ASHP and ACCP directories to get a better idea of the many residency and fellowship opportunities out there and which institute may best suit you.
Whatever you wish to do is ultimately your decision. Reach out to individuals that took a similar career path that interests you. Ask them questions that will guide you to understand if the career path you are interested in is the right one for you. In today’s world of career networking through social media platforms like LinkedIn, pharmacists can provide you with valuable feedback on why they chose their own journeys and how their choices have impacted their lives over the years. It is crucial to keep seeking advice from other pharmacists who have been where you want to go. Striving for excellence is what we pharmacists know how to do quite well. All we recommend from our end is to be the best version of yourself and manifest all your skills in an effort provide to the pharmacy profession.
Good luck!
Dagmara Zajac
RxPharmacist Team
References:
Dang, Y. H., To-Lui, K. P. (2020). Pharmacist perceptions of and views on postgraduate year 3 training. American Journal of Health-System Pharmacy, 77(18), 1488-1496. doi:10.1093/ajhp/zxaa198
Goode, J. R., Owen, J. A., Bennett, M. S., & Burns, A. L. (2019). A marathon, not a sprint: Growth and evolution of community-based pharmacy residency education and training. Journal of the American College of Clinical Pharmacy, 2(4), 402-413. doi:10.1002/jac5.1140
After finding out about the RxPharmacist Graduate Transitions Program through my school advisor, I had a strong interest in joining the program. I definitely thought it was too good to be true, to earn income while studying for your boards, but it has truly been a mutually beneficial experience! With a fellowship position already in place, I wanted to join the summer internship to enhance my work experiences and further build my skillset before beginning my fellowship in July. The program is very unique in that it specifically caters to graduating fourth year students and gives them an opportunity to edit or create MPJE/NAPLEX material of the student’s interest. Since I attended pharmacy school in Florida, I had no experience with the Massachusetts MPJE material, but I wanted to be licensed in the state for my fellowship. After editing the Massachusetts guide, I found the whole experience to be very effective and helpful in learning the material. I feel very prepared to take my MPJE exam and pass on the first time easily.
The RxPharmacist Graduate Transitions Program is very flexible and really cares about the success of the intern. I was able to create my own schedule and work on my own time. Throughout the program, I have learned valuable skills through the workshops offered on topics such as LinkedIn and writing effective cover letters through RxPharmacist’s, “How to get a Job Series” program that all interns get free access to. I have also expanded on my previous writing experiences that I know will be very beneficial to my career in the pharmaceutical industry. Another perk of the program is being matched with a mentor to support you through your projects and help you further your professional development. I enjoyed my sessions with my mentor and being connected with other professionals within the pharmaceutical industry. I cannot recommend this program enough, you need to definitely apply!
I stumbled upon RxPharmacist from a dear friend of mine who kindly forwarded the email she received about their internship programs over to me. I remember taking a quick glance out of confusion then rereading everything as it sounded too good to be true! It turns out I was right, it WAS too good to be true! RxPharmacist has a noble mission of not only helping pharmacy students pass their boards, but also earn some cash in the process. On top of everything, there are optional sessions for career growth, mentorship, and interviewing tips. For me, this was a once in a lifetime opportunity that helped me answer some of my own dilemmas and pursue my true passion. Questions such as should I pursue a regular pharmacist job out of graduation, or can I be able to strive for an entry level position in the pharmaceutical or medical writing industry? After all, the skills you gain here will take you as far as you let them. This internship program by RxPharmacist is designed to help each one of us [the interns] establish a solid foundation that will set us apart in today’s competitive workforce.
My favorite part about this internship is the flexibility you are given when it comes to balancing your schedule. This is beneficial as I felt that I needed to practice having more of a “work-life balance” and there was no better way of doing so than with a fully remote work environment. RxPharmacist has been doing 100% remote work since 2016! For anyone seeking a non-traditional pharmacy role, this is the way to go as it may help some people realize if this path is even right for them and discover what they truly want out of a job and their life. This is why I highly recommend this internship for anyone seeking to challenge themselves, help future pharmacists, and gain new skills in a relatively short amount of time. Reflecting on my experience, I have learned more about my work and learning styles, as well my inspirations. I am more driven than ever to achieve my goals thanks to this exclusive experience I shared with my mentors and fellow interns. I hope that anyone out there who feels lost or unsure of what the future holds for them after pharmacy school explores this unique opportunity to experience it for themselves.
Current Trends During the COVID-19 Pandemic and the Pharmacist’s Perspective
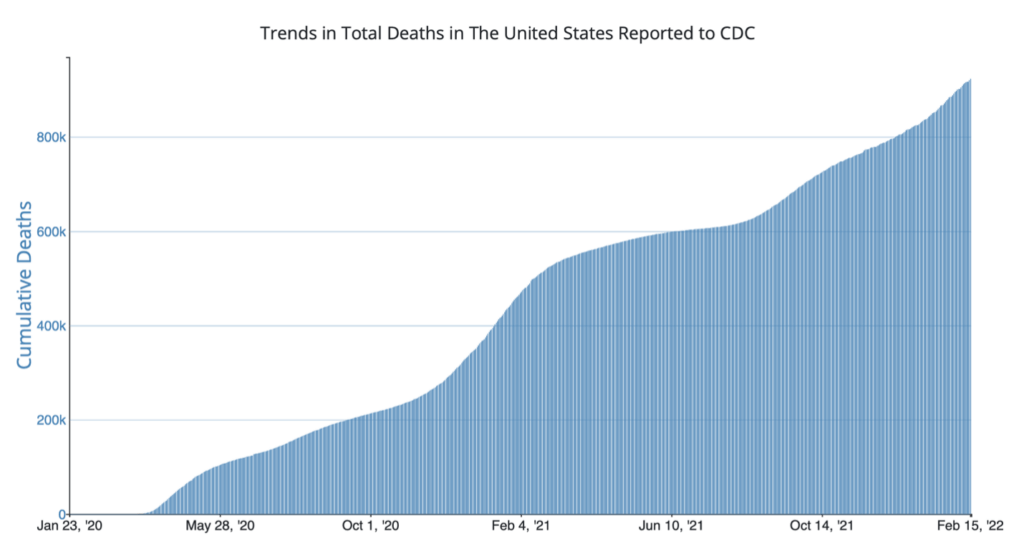
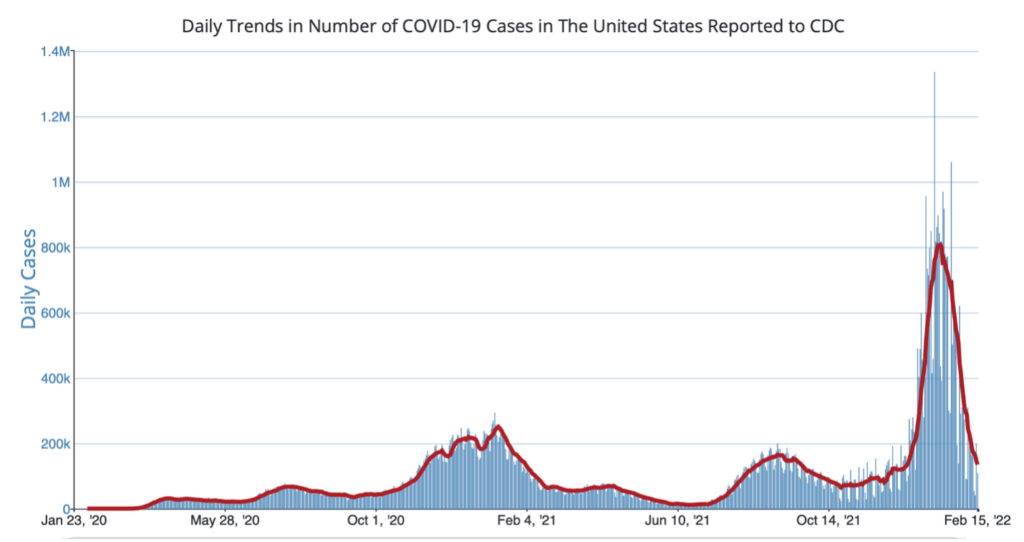
The COVID-19 pandemic has affected everyone at some point. From job displacement to the loss of a loved one, COVID-19 has definitely changed the way we function in society. As some states are adopting to relax COVID-19 masking policies, the pandemic that began two years ago is not over yet. The CDC estimates that over 930,000 people in the United States have died from COVID-19.1 As we approach the unfortunate million number milestone, there are an estimated 130,000 weekly cases of COVID-19 as of February 2022.1
Some challenges that we have seen during these trying times have been especially taxing for healthcare professionals. Surges in COVID-19 hospital admissions, medical staff shortages, and usually long hours behind the pharmacy counter have left some providers with a sense of mental burnout. As a result, the “great resignation” has led numerous people to jump ship from their current jobs in search of finding that work-life balance that many once had prior to the pandemic. Some retail pharmacists are even moving to nontraditional careers such as remote opportunities amid the shortages of help and reduction of pharmacy store hours.2,3,4 Some common stressors pharmacists face are listed in the chart below.
Common COVID-19 Stressors Pharmacists Experience5
Facing Uncertainty
Staffing Issues
Increased Workload
PPE Shortages
Updated/Changing Guidelines
Family Health Concerns
Lack of Role Clarity
Threat to Professional Identity
PPE = Personal Protective Equipment
On the other hand, roles for pharmacists, pharmacy students, and pharmacy staff have greatly expanded throughout the COVID-19 pandemic, creating a kind of incentive for pharmacists to provide vital and necessary patient care.6 Some examples of these role expansions have been:
Creating community pharmacies that serve as COVID-19 testing sites
Permitting emergency pharmacist authority for pharmacist refilling (in some states)
Allowing pharmacy student volunteering while under pharmacist supervision
Granting pharmacy technicians the rights to administer vaccines, conducting remote data entry tasks, and taking new orders (in some states)
Image: unsplash.com
The Pharmacist’s Role Concerning Vaccinations, Home Testing Kits, and Personal Protective Equipment
The general public who visit the pharmacy may have several questions or reservations concerning COVID-19 vaccines. We’ve all seen and heard the vast amounts of misinformation regarding vaccines out there on social media, and it is important for pharmacists to intervene and educate patients about certain misconceptions. The public may ask these questions for themselves, for their family members, or for their own children. Some common COVID-19 vaccination concerns are outlined below. For more information regarding frequently asked vaccination questions, please refer to the CDC website.
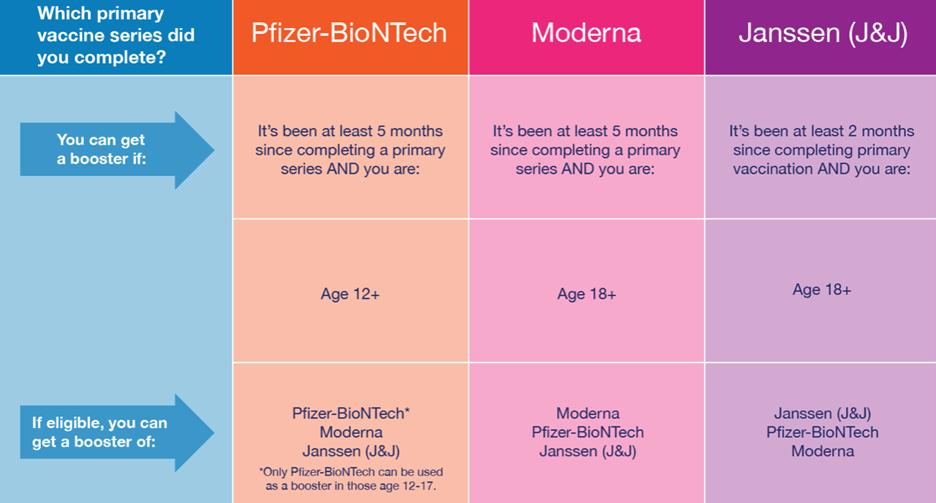
In recent news, Pfizer-BioNTech (Comirnaty®) and Moderna (Spikevax) COVID-19 vaccines have been approved by the FDA for the prevention of COVID-19 and authorized for emergency use.7,8 The Janssen (Johnson & Johnson) COVID-19 vaccine, however, does not yet have FDA approval but is authorized for emergency use.9
Each vaccine has different criteria (e.g., age, booster eligibility) for patients. If a patient is receiving their COVID-19 vaccination for the first time, it would be wise to go over the vaccination schedule with them to ensure proper follow up. So far, most individuals qualify for the normal vaccination series and a booster (See chart below). Currently, the push for a second booster is reserved for individuals who are severely immunocompromised per CDC updates.
In early 2022, the Biden-Harris Administration began the initiative to provide millions of Americans with free at-home COVID tests and N95 masks. This decision came after massive surges in COVID-19 cases and when the Centers for Disease Control’s updated its guidance on N95 masks, noting that these masks offer “the highest level of protection.”10
In pharmacies today, people are eligible for free at-home COVID-19 testing kits with or without insurance plans. Everyone is now able to claim at least 4 at-home tests per household. Pharmacists can direct the general public to this government website for free orders. Kits usually arrive in about 7 to 12 days and is delivered by the United States Postal Service. For information on N95 mask availability, individuals are advised to contact their local grocery stores, pharmacies or community centers.
The Pharmacists Role in Advocating Mental Health
From day to day, pharmacists might be overwhelmed and preoccupied with consults, phone calls, medication reconciliations, issues with prior authorizations, or medication transfers to say the least. Understandably so, this makes sense since there are so many tasks to do in a short amount of time. Even though a great deal of work is handled behind the scenes, it is important to recognize situations where patients or even coworkers might need certain help, especially when it comes to mental health.
Incidences of depression have unfortunately been on the rise during the pandemic. In a longitudinal study that followed groups of U.S adults 18 years and older from March-April of 2020 and March-April 2021, depression in representative samples showed an increasing trend.11 In this study, the 2020 March-April cohort reported 27.8% depressive symptoms (95% CI: 24.9, 30.9) while the 2021 March-April cohort reported 32.8% depressive symptoms (95% CI: 29.1, 36.8). Reasons for the recent increases in depression have been attributed to life stressors such as socioeconomic status and job loss.11
depressed mood or loss in interest in things that are pleasurable
concentration disturbances
energy loss
psychomotor agitation or slowing
If the pharmacist has reason to believe that an individual might be suffering from depression, they can offer suggestions or recommendations to assist others. Mental health stigma is still very much widespread and negative societal beliefs may prevent others from seeking any help at all. It is always important however, to approach mental health discussions with a welcoming, yet careful manner to open up conversations that might be uncomfortable at first. Referring someone to a provider, therapist, or counselor is a great start. For more resources, visit the National Institute of Mental Health website.
Common resources utilized for immediate intervention are the following:
Pharmacists everywhere can do their part to help those who need it the most during the COVID-19 pandemic. For pharmacists who have stayed diligent in providing continued, exceptional healthcare during the pandemic, their role in helping patients has never been more crucial. Even though time constraints during the pandemic may be the biggest barrier in helping patients throughout the day, pharmacists can still exercise their judgements in helping patients who may need that extra care. Although we may not know what changes to expect during this pandemic, we can certainly adapt to provide exceptional healthcare to everyone.
Dr. Joseph Suarez, Pharm.D. is a Medical Writer at RxPharmacist, LLC who resides in San Antonio, Texas. His interests are in psychopharmacology, psychotherapy, and reconciling healthcare disparities. Dr. Suarez is seeking opportunities to utilize his incredible medical writing talents. If you are looking to hire, you may contact Dr. Suarez via LinkedIn.
Langran C, Mantzourani E, Hughes L, Hall K, Willis S. “I’m at breaking point”; exploring pharmacists’ resilience, coping and burnout during the covid-19 pandemic. Exploratory Research in Clinical and Social Pharmacy. 2022;5:100104. doi:10.1016/j.rcsop.2022.100104
Merks P, Jakubowska M, Drelich E, et al. The legal extension of the role of pharmacists in light of the COVID-19 Global Pandemic. Research in Social and Administrative Pharmacy. 2021;17(1):1807-1812. doi:10.1016/j.sapharm.2020.05.033
Comirnaty® [package insert] Pfizer Inc., New York, NY. 2021.
Spikevax [package insert] Moderna US, Inc. Cambridge, MA, 2022.
Janssen. [package insert] Janssen Biotech, Inc. A Janssen Pharmaceutical Company of Johnson & Johnson Horsham, USA, PA. 2021.
Ettman CK, Cohen GH, Abdalla SM, et al. Persistent depressive symptoms during COVID-19: A national, population-representative, Longitudinal Study of U.S. adults. The Lancet Regional Health – Americas. 2021;5:1-12. doi:10.1016/j.lana.2021.100091
All images in this article pulled from: unsplash.com
PTSD Overview
Post-traumatic stress disorder (PTSD) is a type of anxiety disorder that is more common than you might think. It is estimated that at least 60% of men and 50% of women will go through some sort of traumatic experience in their lifetime.1 Also, the one-year prevalence of PTSD in the United States is approximately 3.5 to 4.7 percent.2 PSTD has long been associated with the terms “shell shock,” “post-Vietnam syndrome,” and “combat fatigue” in veterans for years; however, PTSD can occur in all populations regardless of age, gender, race, or socioeconomic status.3 There are many treatments available for PTSD that have been proven effective and in recent years, there have also been innovative yet experimental approaches to treating PTSD.
In summary, PTSD occurs after a traumatic experience (e.g., car collision, sexual assault, witnessing a death, developing a serious medical illness) and can manifest in different ways months to years after the trauma has passed. Although every case of PTSD is unique, many people will experience hallmark symptoms or manifestations such as intrusion, hyperarousal, avoidance,and distortions in thinking. These symptoms must be present for at least a month and cause marked distress that impairs the person’s quality of life.3
PTSD Symptoms/Manifestations3
Term
Definition
Examples
Intrusion
Unwanted and intrusive thoughts associated with trauma. This is also known as “re-living” the traumatic experience and can occur with constant flashbacks or nightmares. Certain noises, sights, and smells of a similar manner in which the trauma occurred can trigger strong, spontaneous emotions.
A retired veteran wakes up from a recurring nightmare about an airstrike that occurred 30 years agoA woman has an instant flashback of a robbery that happened a year ago while hearing popping of balloons in a department store
Hyperarousal
The state of being irritable, easily shaken, hypervigilant, self-destructive, distracted, or unreasonably aggressive after a traumatic experience occurs.
A young man becomes overprotective of his 5-year-old daughter around dogs after a he suffered a vicious dog attack last month A woman flinches when people hug her during get-togethers after a close family friend sexually assaulted her years ago
Avoidance
Evading or going out of one’s way to avoid situations, places, discussions, activities, or objects that serve as triggers of past trauma.
A man takes a shortcut on his way to work to avoid the construction site where he crashed into another car during a busy intersectionA girl avoids rollercoasters when she goes to amusements parks after her friend was ejected next to her on a ride with faulty safety equipment
Distortions in Thinking
Irrational, distorted, or negative thinking in one’s behavior, feelings or thoughts after experiencing trauma. This can lead to beliefs that oneself or other people are “untrustworthy” or “bad.” Sometimes there is also thinking that oneself or other people do not deserve happiness or the right to lead a normal life.
A woman holds anger directed at all of her doctors after learning her primary care physician misdiagnosed her serious heart condition that caused a delay treatmentA man cuts off all communication with his friends and family after he was robbed at knifepoint while walking to the bus stop two years ago
As always, it is important that proper diagnosis from either a psychiatrist, physician assistant, nurse practitioner, or licensed therapist is confirmed before any treatments are started. Related conditions that can highly mimic PTSD are the following3:
social anxiety disorder
panic disorder
agoraphobia
separation anxiety disorder
social anxiety disorder,
acute stress disorder,
disinhibited social engagement disorder, adjustment disorder
reactive attachment disorder (in children)
Image: unsplash.com
Current Evidenced-based Treatments for PTSD
There are a wide array of treatments for PTSD that are backed by evidence-based science. PTSD patients can choose nonpharmacological, pharmacological, or a combination of both. At times patients can be hesitant to try a new medication and might want to explore other approaches first. Since patient situations and circumstances vary, the provider and patient will come up with a plan for the best course of treatment. Nonpharmacological treatments for PTSD psychotherapies involve cognitive behavioral therapy (CBT). The types of CBT that are promoted by the American Psychological Association (APA) guidelines and the Veterans Health Administration and Department of Defense (VA/DoD) guidelines are4,5:
Cognitive Processing Therapy(CPT) – A type of PTSD therapy that focuses on changing internal thoughts and feelings in order to eliminate current and future negative thoughts and actions. CPT encourages the patient to rationalize or “make sense” of the traumatic experience, and how it has changed their perceptions either about themselves or others around them. CPT is typically 12 sessions (once weekly) and the patient will learn tools to help them come to terms with their trauma and how to cope with everyday life.6
Prolonged Exposure (PE) – A type of PTSD therapy that involves “rechallenging” or gradual repeated exposure to a situation, place, or activity that was once the source of trauma for the patient. PET helps the patient to incorporate “emotional processing” to slowly process the events related to the trauma that was not processed initially. To help guide this process, in vivo and imagined exposure are incorporated into therapy. In vivo exposure encourages patients to go back to the event, situation, or activity to accomplish a sense of desensitization of the trauma. Imagined exposure helps patients with confronting thoughts, memories and feeling surrounding the traumatic experience.6
Image: unsplash.com
Another psychotherapy treatment for PTSD is Eye Movement Desensitization Reprocessing (EMDR). This involves the patient recalling the trauma and examining the patient’s current emotional state. The patient moves their eyes from side to side during the session and the patient slowly incorporates positive thoughts when the traumatic thoughts subside.6
The APA and the VA/DoD have recommended CPT and PE after extensive systematic and meta-analysis of these evidenced-based treatments.7 It is important to note that the APA guidelines on PTSD are for treating all individuals, while the VA/DoD guidelines are recommendations for providers working for the VA or the DoD.7 Currently the APA guidelines suggests the use of EMDR, however the level of evidence is conditional.4 It is unclear at this time if the level of evidence will be changed to “strong” in the not-too-distant future. This contrasts with the VA/DoD’s strong recommendation for use in patients with PTSD.5 Even though EMDR needs additional exploration to address some limitations (cultural differences, diverse clinical settings), EMDR is still widely used in patients with PTSD.7
Image from unsplash.com
Pharmacotherapy
Currently, only four medications are recommended for the treatment of PTSD: sertraline, paroxetine, fluoxetine, and venlafaxine. While only sertraline and paroxetine are FDA approved for the treatment of PTSD, the APA and the VA/DoD recommend all the aforementioned medications for use.4,5
Medication Recommendations for PTSD4,5,8
Medication/Class
Indication
FDA Approval
APA Recommendations
VA/DoD Recommendations
Sertraline (SSRI)
PTSD
Yes
Conditional*
GRADE A†
Paroxetine (SSRI)
PTSD
Yes
Conditional
GRADE A
Fluoxetine (SSRI)
PTSD (off-label)
No
Conditional
GRADE A
Venlafaxine SNRI)
PTSD (off-label)
No
Conditional
GRADE A
SSRI = Selective Serotonin Reuptake Inhibitor, SNRI = Serotonin-Norepinephrine Reuptake Inhibitor, * = Conditional recommendation indicates good outcomes, but evidence may not be robust (risks vs benefits may vary from patient to patient), † = The GRADE system examines four domains for strength recommendation: Outcomes (morbidity, mortality, quality of life), Evidence Quality (randomized controlled trials, meta-analysis), Patient Preferences (risks vs benefits for patients, certain beliefs or perspectives in approach to therapy) and Other Implications (resources and/or cost-effectiveness)
In patients with PTSD, the VA/DoD suggests the usage of trazodone (GRADE B evidence for adjunctive treatment) for sleep disturbances and prazosin (GRADE B evidence for adjunctive treatment) for nightmares. Currently, the APA does not have current recommendations for these medications two medications.4,5
As far as benzodiazepines are concerned, the APA does not make mention of any usage of this medication class in their guidelines. The VA/DoD however, strongly recommends (GRADE D) against the usage of benzodiazepines, citing insufficient evidence and adverse side effect profiles5,9
Image: unsplash.com
The Future of PTSD Treatments: Psychedelics
Recently, the use of psychedelic medications has been gaining worldwide attention. In 2019, esketamine, a dissociative hallucinogenic therapy, was approved by the FDA for treatment-resistant depression.10 Other psychedelics such as psilocybin and 3,4-methylenedioxymethamphetamine (MDMA) have also followed suit for future FDA approval.
In 2021, psilocybin was granted FDA breakthrough therapy designation for depression after a phase 2, randomized, double-blind, placebo controlled trial.11 This trial compared baseline depression scale scores in those taking either escitalopram or psilocybin.12 Results showed little difference in the change in scores (2 points difference between both groups) but did implicate some promise for future use. Experts claim that psilocybin will likely gain FDA approval for depression in a couple of years.13 In the PTSD realm, the jury is still out on whether or not psilocybin has its own unique place in therapy.
Similarly, MDMA was granted FDA breakthrough therapy designation for the treatment of PTSD first in 2017 after a phase 2 trial, and more notably in 2021 after a phase 3, randomized, double-blind, placebo controlled trial.14,15The 2021 phase 3 trial compared the remission rates of PTSD in those taking either MDMA or placebo. After 18 weeks, two-thirds (67%) of the participants taking MDMA demonstrated complete remission of PTSD as opposed to the 32% taking placebo.10 Even though head-to-head studies are needed to demonstrate superiority (sertraline vs MDMA), so far, this novel treatment is making strides on its own.15 FDA approval for the use of MDMA in patients with PTSD could be coming as soon as 2023.13
Possible uses of psilocybin and MDMA does come with its own disadvantages. Both medications do carry the potential for abuse, just like their predecessor esketamine. Another thing to consider is the limitations of the setting in which these psychedelics are taken. In other words, it is highly unlikely that both these medications will be administered in a place other than a controlled environment like a licensed facility.
Whether we want to accept it or not, psychedelics might be here to stay for the long haul. What was once viewed by many as dangerous, mind-altering drugs are now seen with gradual acceptance for the future in treating many mental illnesses including PTSD.
About the Author
Dr. Joseph Suarez, Pharm.D. is a Medical Writer at RxPharmacist, LLC who resides in San Antonio, Texas. His interests are in psychopharmacology, psychotherapy, and reconciling healthcare disparities. Dr. Suarez is seeking opportunities to utilize his incredible medical writing talents. If you are looking to hire, you may contact Dr. Suarez via LinkedIn.
Clinical Practice Guideline for the Treatment of PTSD. American Psychological Association. https://www.apa.org/ptsd-guideline/ptsd.pdf. Published February 24, 2017. Accessed February 1, 2022.
Watkins LE, Sprang KR, Rothbaum BO. Treating PTSD: A review of evidence-based psychotherapy interventions. Frontiers in Behavioral Neuroscience. 2018;12(258).doi:10.3389/fnbeh.2018.00258
Medications for PTSD. American Psychological Association. https://www.apa.org/ptsdguideline/treatments/medications. Published May 2017. Accessed February 1, 2022.
Carhart-Harris R, Giribaldi B, Watts R, et al. Trial of psilocybin versus escitalopram for depression. New England Journal of Medicine. 2021;384(15):1402-1411. doi:10.1056/nejmoa2032994
Expert: MDMA is very likely to be FDA-approved for PTSD by the end of 2023. Pharmacy Times. https://www.pharmacytimes.com/view/expert-mdma-is-very-likely-to-be-fda-approved-for-ptsd-by-the-end-of-2023. Published November 7, 2021. Accessed February 1, 2022.
Feduccia AA, Jerome L, Yazar-Klosinski B, Emerson A, Mithoefer MC, Doblin R. Breakthrough for trauma treatment: Safety and efficacy of MDMA-assisted psychotherapy compared to Paroxetine and Sertraline. Frontiers in Psychiatry. 2019;10.doi:10.3389/fpsyt.2019.00650
Mitchell J, Harrison C, Lilienstein A, Bogenschutz M. MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled phase 3 study. Nature Medicine. 2021;27:1025-1033. doi:https://doi.org/10.1038/s41591-021-01336-3