During my final year of pharmacy school, I had the unique opportunity to join the RxPharmacist team as a medical writing intern. I was particularly drawn to this role because it aligned well with my passion for education and my interest in the test prep industry. First, my experiences in various tutoring and mentoring roles taught me how impactful it can be to equip patients and students with the knowledge they need to achieve their individual goals. Second, I believe that accessible, digestible education is key, and that medical writing is an effective medium to provide it. As such, the internship program offered by RxPharmacist stood out to me because it provided an opportunity to improve my medical writing skills, which are important for both pharmacists and educators, while giving back to the pharmacy community.
RxPharmacist is a company that is deeply invested in the academic and professional success of students. They offer a multitude of up-to-date, high-quality test prep guides and resources that equip students to excel in diverse environments beyond the classroom. Driving this company is a team that works harmoniously together and continuously innovates to improve the quality of their services. I had the privilege of working with this dedicated team when creating a test prep guide for the Pharmacy Technician Certification Exam (PTCE), where I received expert guidance and encouragement that helped me grow both personally and professionally.
During my internship, I gained valuable hands-on experience developing a book, designing an online course, and writing mock exam questions. Balancing the creation of the test prep guide with my APPE rotations was undoubtedly challenging, but it significantly improved my time management, communication, and organizational skills. Moreover, I have become more confident in my medical writing abilities, as I am able to present complex concepts clearly and concisely. The skills I refined, including researching and extracting pertinent information from reliable resources, tailoring my writing to specific audiences, and presenting details with clarity, position me for success as I continue to develop as an effective clinician and educator.
As an intern, I also participated in the “How to Get a Job” training series, which allowed me to gain insight into the importance of networking, managing finances, negotiation, and other critical skills needed to navigate the job market and attain professional success. This series provided practical modules packed with high-yield strategies to help users maximize the potential of their degrees. Thanks to this series, I emerged feeling more confident about crafting a strong CV and interviewing. I would highly recommend this resource to any pharmacy student interested in pursuing a fellowship, residency, or other career path.
I am incredibly grateful for the opportunity to hone my skills as a medical writer under the guidance of the talented and passionate team at RxPharmacist. Serving as an intern was a transformative journey that has prepared me to make meaningful contributions to the pharmacy profession and beyond. I would wholeheartedly recommend this internship to students interested in professional development and gaining hands-on experience in medical writing while working with a supportive team.
As an intern at RxPharmacist, I have experienced significant personal and professional growth. This internship has provided me with the opportunity to dive deep into areas of pharmacy that I may not have been exposed to during my academic coursework. I gained a better understanding of the behind-the-scenes work that contributes to the development of medical resources and educational tools that benefit not only pharmacy professionals but also the broader healthcare community. The major focus of my internship was strengthening my understanding of the core principles behind medical writing, which is an essential skill for anyone looking to pursue a career in the pharmaceutical industry. Throughout my internship, I had the opportunity to work on several projects that involved creating educational materials, writing study guides, and simplifying complex pharmacy law concepts.
One of the most valuable lessons I learned was the importance of clarity and precision when writing about medical and legal topics. Medical writing requires a delicate balance between accuracy and readability, as these concepts must be easily understood by both professionals and students alike. The ability to communicate complicated ideas in a straightforward manner is crucial in ensuring that the information reaches its intended audience effectively. Simplifying complicated pharmacy law concepts, in particular, was a challenge that pushed me to refine my communication skills. Pharmacy law, with its detailed regulations and legal jargon, can often seem overwhelming. However, by breaking down these intricate regulations into digestible pieces, I was able to better appreciate the technicalities of pharmacy law while also contributing to the development of resources that would be valuable to others. This experience allowed me to further develop skills that will be indispensable throughout my career.
Another important aspect of my internship at RxPharmacist was the mentorship I received from my preceptor and the executive team at RxPharmacist. My preceptor’s guidance and constructive feedback were instrumental in helping me refine my writing and improve my overall approach to medical writing. Their mentorship was invaluable, providing me with the tools and confidence needed to succeed. Similarly, the leadership team exemplified their dedication to the company’s mission created an environment where us interns could thrive. The information shared in the “How to Get a Job Series” was very insightful and will be beneficial in many years to come. The RxPharmacist team was always willing to provide advice, answer questions, and share their wealth of knowledge, which greatly enhanced my learning experience.
Overall, my time at RxPharmacist has been incredibly rewarding, and I am deeply grateful for the opportunity. One of the most rewarding aspects of my internship was the chance to collaborate with a diverse group of individuals, each bringing unique perspectives and expertise to the table. This allowed me to gain new insights, learn from others’ experiences, and broaden my professional network. Working alongside experienced professionals has not only helped me apply the skills I have learned in pharmacy school but also provided me with hands-on experience that will benefit me in the future. This internship taught me how to approach problems from different angles, prioritize tasks effectively, and communicate with a variety of audiences.
I am confident that the skills and insights I gained during this internship will continue to shape my professional journey as I move forward in my career. I now feel better prepared to tackle future challenges in the pharmacy field and contribute meaningfully to the healthcare community. My time at RxPharmacist has helped me develop critical thinking skills, enhanced my writing abilities, and provided me with a deeper understanding of pharmacy law and medical writing.
I would like to extend my heartfelt thanks to everyone at RxPharmacist for providing me with this memorable and enriching opportunity. I would highly recommend this program to any pharmacy student who is looking to challenge themselves beyond the typical curriculum. The experience at RxPharmacist offers hands-on learning, mentorship, and the chance to contribute meaningfully to real-world projects. It is a great way to enhance your knowledge and skills, while also gaining a deeper understanding of the many facets of the pharmacy profession. The lessons learned and experiences gained will undoubtedly have a lasting impact on my career, and I am grateful for the opportunity to be part of such a dynamic and supportive team.
-Chloe G., Wilkes University PharmD Candidate 2025
“I also had the chance to work with members of the RxPharmacist team to clarify my personal brand and improve my networking, interviewing, and job offer negotiation skills.”
I recently completed an APPE rotation with RxPharmacist. As someone with no experience in medical writing and a limited understanding of what medical writers do, I am not sure what motivated me to choose this APPE rotation. However, after spending 5 weeks learning from the RxPharmacist team I can say I am very happy with my choice.
For the first part of this rotation, I updated the Minnesota MPJE study guide. This was the perfect start to my medical writing journey as I was able to use the previous edition of the study guide to direct my writing. My preceptor guided me through state and federal law updates as well as how to write the best MPJE practice questions! I received thoughtful feedback throughout the process that helped me develop a product that I am proud of.
The second half of my rotation focused on creating blog posts about a variety of pharmacy topics. This challenged me to expand my writing knowledge and to practice condensing complex pharmacy topics into short, understandable posts. I had the freedom to choose topics that interested me which made the whole process very enjoyable. It was a great way to review core pharmacy information from my pharmacotherapy courses while practicing medical writing. My preceptor provided helpful feedback that improved the clarity of each of the blog posts I wrote. She also gave me an overview of the different types of medical writing and shared many of the places medical writing and pharmacy overlap.
As a bonus, I also had the chance to work with members of the RxPharmacist team to clarify my personal brand and improve my networking, interviewing, and job offer negotiation skills. While this was not directly related to medical writing, it was yet another valuable piece of this rotation.
Here are my top 3 takeaways:
There is something for everyone, whether you want to work on creative writing or dig into state laws.
Everyone can benefit from learning more about medical writing, regardless of past writing experience.
It is fun to take a break from direct patient care while still focusing on pharmacy topics!
Completing an APPE with RxPharmacist taught me skills that I would not have learned through other APPE rotations. I would recommend this rotation to all pharmacy students regardless of the pharmacy career they are aiming for. I believe that the experience I gained will help me with upcoming job applications and interviews as well as in my day-to-day work as a pharmacist.
Human immunodeficiency virus (HIV) is a retrovirus that can lead to acquired immunodeficiency syndrome (AIDs) if left untreated. Almost 40 million people worldwide have HIV and 630,000 people died from HIV in 2023. HIV attacks the immune system by targeting white blood cells. Patients infected with HIV are more likely to contract diseases such as tuberculosis and cancer due to their decreased immune function. Currently, there is no cure for HIV, but many medications exist to treat HIV and prevent its spread. The long-term effectiveness of these medications is directly related to patient adherence and treatment resistance. Long-acting injectable medications may be a good option for patients who struggle with adherence to daily oral treatments.
What was the FLAIR trial?
The FLAIR trial was a randomized, open-label, noninferiority trial taking place in multiple treatment centers. It aimed to prove noninferiority of an injectable two-drug antiviral regimen versus an established oral three-drug antiviral regimen in patients who had never received treatment for HIV.
The experimental medication, now known as Cabenuva, is a long-acting treatment containing two medications, both of which were individually FDA-approved for the treatment of HIV prior to this trial. The first is cabotegravir, an integrase strand-transfer inhibitor (INSTI). INSTIs work by blocking the integration of viral DNA, stopping the replication of HIV. The second medication is rilpivirine, which is a nonnucleoside reverse-transcriptase inhibitor (NNRTI). NNRTIs work by inhibiting HIV-1 transcriptase which prevents HIV replication. In this trial, Cabenuva was given as an intramuscular injection once monthly.
The comparator treatment was a standard HIV treatment regimen, containing three oral antivirals: dolutegravir, abacavir, and lamivudine. This combination is taken once daily and represents a guideline-recommended treatment option for HIV.
The goal of HIV treatment is to reduce morbidity and mortality as well as decrease the spread of HIV. Antiviral medications are used to reduce a patient’s viral load to an undetectable level, which prevents HIV transmission. As defined by the CDC, antiviral treatment that results in a viral load of < 200 copies per mL is considered to be successful.
How was the study conducted?
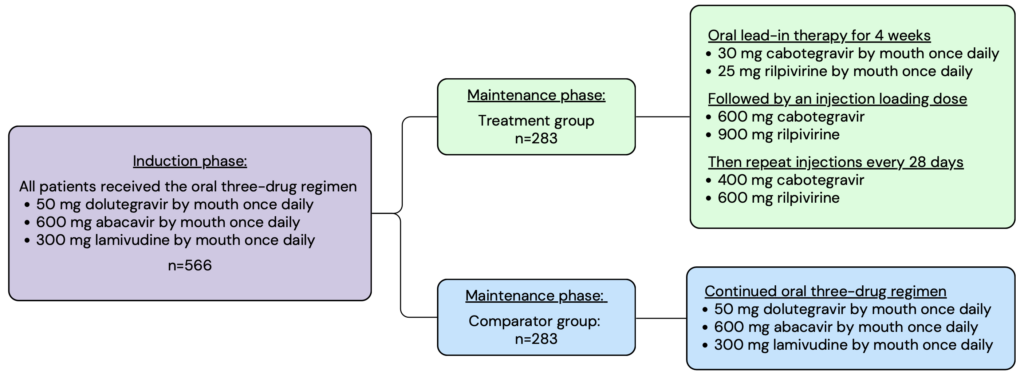
The FLAIR trial contained two main phases, the induction phase and the maintenance phase. In the induction phase, all enrolled patients were given the three-drug oral regimen daily for 20 weeks. After 16 weeks, patients underwent additional testing to ensure that their viral load was less than 50 copies per mL. Patients who met the criteria continued to the maintenance phase where they were randomized into either the experimental or comparator treatment group. Members in the experimental group were given an oral lead-in of daily cabotegravir and rilpivirine, followed by a loading dose injection, and then continued with the monthly injectable maintenance dose thereafter. Members in the comparator group continued on the daily three-drug oral regimen. The intention-to-treat population was analyzed with a total of 566 patients split evenly between the two treatment groups.
Image created with Canva
Patients included in the FLAIR trial had to have active HIV, as determined by a plasma screening, that had never been treated with antiviral medications. This is because resistance is common in patients who have previously been treated with antiviral medications. To avoid complicating the results, the trial only included patients who had no history of antiviral use and therefore had the lowest likelihood of treatment resistance. Patients were excluded from this trial if they could not take antiviral medications due to their comorbid health conditions.
Notable inclusion criteria:
HIV infection that has never been treated with antiviral medications
HIV RNA level ³ 1000 copies per mL
18 years old or older
Notable* exclusion criteria:
Anyone who was pregnant or breastfeeding
Patients with active Stage 3 disease as defined by the CDC
Hepatic impairment
Current or previous hepatitis B infection
*This list includes highlights from the patient enrollment parameters. It does not include all exclusion criteria.
The primary endpoint measured during this trial reflects the ability of the long-acting treatment and comparator medications to provide viral suppression, which is the main goal of HIV treatment. This was defined as the percentage of participants with a plasma HIV RNA level of ³ 50 copies/mL at week 48.
The secondary endpoints provide additional data regarding treatment effectiveness, adverse events, and pharmacokinetics. The key secondary endpoint measured was the percentage of patients with a plasma HIV RNA level of < 50 copies/mL at week 48.
Some additional secondary endpoints included:
Virologic failure
Adverse events
Plasma pharmacokinetics
Adherence
The intention-to-treat population was statistically analyzed. The adjusted difference between the treatment and comparator groups was determined for the primary and secondary endpoints using a stratified Cochran-Mantel-Haenszel analysis. Based on the power of the study and the size of each study group, noninferiority for the primary outcome was proven if the difference between the two groups was less than 6 percentage points.
Outcomes of the trial
The primary endpoint occurred for 6 patients in the Cabenuva group and 7 patients in the comparator group. This was a difference of -0.4 percentage points, demonstrating noninferiority of the study drug.
The key secondary endpoint occurred in 93.6% of patients in the Cabenuva group and 93.3% of patients in the comparator group, also demonstrating noninferiority of the treatment group with an adjusted difference of 0.4 percentage points (95% CI: -3.7 to 4.5).
Adverse events were more common in the Cabenuva group (94%) versus the comparator group (80%). The most common side effect of Cabenuva was injection site reaction, occurring in 86% of patients. Injection site pain accounted for most of these and was most commonly characterized as mild in severity. After the initial injection, 71% of patients reported injection-site reactions, and at week 48, the prevalence dropped to 20% of patients who received the trial medication. Additional common adverse effects included headache, diarrhea, and upper respiratory tract infection.
The FLAIR trial showed noninferiority of Cabenuva, a long-acting injectable medication when compared to a three-drug oral regimen to treat HIV. Cabenuva achieved similar rates of viral suppression for patients who had not previously been treated with antivirals for HIV. However, it also had higher rates of adverse effects. These were most commonly injection site reactions, which can be accounted for by the difference in the route of administration.
Another clinical trial, the ATLAS trial, studied the efficacy of Cabenuva in patients who had been successfully treated for HIV with antivirals in the past. Similar outcomes were reported for both the FLAIR and ATLAS trials. These two trials provided data supporting the efficacy of Cabenuva in viral suppression for patients with HIV regardless of their previous antiviral use.
Barriers to successful HIV treatment
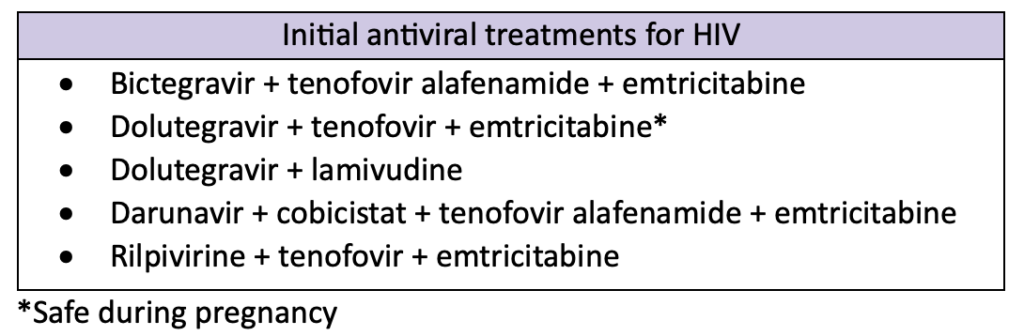
HIV is an extremely complex disease state to treat. Many medications can be used in a variety of combinations to treat patients. The table below outlines a few common first-line treatment recommendations.
Regimens that contain bictegravir or dolutegravir are highly effective and tolerable. They also have a lower pill burden and high barrier to resistance compared to other medications, making them good options for initial HIV treatment. Treatment is extremely patient-specific and should take into consideration a variety of factors, including viral load, previous antiviral use, resistance, concurrent infections, and patient intolerance.
Cabenuva is now part of the HIV treatment guidelines. However, Cabenuva is not currently a first-line treatment option. It should not be used if the patient has any history of treatment failure or resistance to either cabotegravir or rilpivirine. Additionally, Cabenuva is not recommended for initial viral suppression. Patients should undergo successful viral suppression with an alternative treatment regimen before switching to a long-acting injectable medication.
Adherence to antiviral medications is key to HIV treatment. These medications reduce morbidity and mortality for patients as well as prevent the spread of HIV. However, their effectiveness is directly related to patient adherence. Poor adherence increases the risk of resistance to HIV medications, limiting treatment options. Barriers to patient adherence include pill burden, complex dosing, side effects, limited access to care, stigma, poor health literacy, and more. Long-acting injectable medications could improve adherence by eliminating pill burden and reducing complex dosing schedules. However, they come with unique side effects and require monthly appointments for administration.
Treatment resistance is a major problem that occurs with HIV medications. Patients should undergo genotype testing for antiviral resistance before starting treatment. This step is of greater importance for patients who acquire HIV while using pre-exposure prophylaxis (PrEP), because some of the medications for PrEP and HIV treatment overlap. Poor adherence is a common cause of treatment resistance. However, resistance can develop even with perfect adherence. Virologic failure (HIV RNA plasma level > 200 copies/mL) due to treatment resistance often requires patients to switch treatment regimens. As patients acquire resistance to first-line treatments, they may have to switch to more complex regimens.
Pharmacists play an important role in HIV care by educating patients on treatment options and encouraging adherence.
Margaret M., APPE Student
References
Long-Acting Cabotegravir and Rilpivirine after Oral Induction for HIV-1 Infection. The New England Journal of Medicine vol. 382,12 (2020): 1124-1135. doi:10.1056/NEJMoa1909512. Available at: https://pubmed.ncbi.nlm.nih.gov/32130806/. Accessed August 29, 2024.
Antiretroviral Drugs for Treatment and Prevention of HIV Infections in Adults: 2022 Recommendations of the International Antiviral Society – USA Panel. International Antiviral Society. Available at: https://pubmed.ncbi.nlm.nih.gov/36454551/. Accessed August 30, 2024.
Urinary tract infection (UTI) is a broad term, encompassing simple and complex infections of the urinary tract and kidneys. In the United States, 40% of women have at least one UTI in their lifetime. Antimicrobials are the main treatment used for UTIs, but selecting the most appropriate option is complicated by increased resistance rates and patient-specific factors. Pharmacists play an important role in the healthcare team by ensuring that antimicrobial selection is optimal for each patient.
Cystitis vs. pyelonephritis
Cystitis is a UTI, consisting of a bladder or lower urinary tract infection. This is the most common type of UTI and one of the most common indications for prescribing antimicrobials in the United States.
Cystitis can be classified as complicated or uncomplicated.
Uncomplicated cystitis is any UTI that occurs in women who are generally healthy and do not have any abnormalities in the structure or function of their urinary tract.
Complicated cystitis is any UTI that occurs in people who have abnormalities to the structure or function of their urinary tract or have other complicating health problems.
UTIs that occur in men or pregnant women are always considered complicated.
Pyelonephritis is a complicated UTI that involves infection of the kidneys or upper urinary tract. This is less common than cystitis and requires more intense treatment.
Who gets UTIs?
Women are 4 times more likely to get a UTI than men. This is due to women having shorter urethras, and a shorter space between the rectum and urethra, both of which allow bacteria to travel more easily to the site of infection. Cystitis occurs most frequently in women ages 16 to 35 but can happen to anyone at any age. Pyelonephritis occurs in about 15-17 cases per 10,000 females and 3-4 cases per 10,000 males each year. In the United States, an average of 250,000 cases of pyelonephritis occur each year.
Some additional risk factors include:
Abnormal function or anatomy of the urinary tract
Antibiotic use
Diabetes
Diarrhea
First UTI before age 15
New or multiple sexual partners
Menopause
Pregnancy
Old age or dementia
Catheter-use
What causes UTI?
Common pathogens that cause cystitis and pyelonephritis are:
Escherichia coli
Proteus mirabilia
Klebsiella pneumonias
Staphylococcus saprophyticus
Enterococcus
E. coli is the most common pathogen in UTIs, responsible for 75-95% of infections. One possible mechanism for the success of E. coli is the p-fimbriae appendages that adhere to epithelial cells in the urinary tract. This can prevent E. coli from being flushed out of the urinary tract, instead giving them time to colonize and spread.
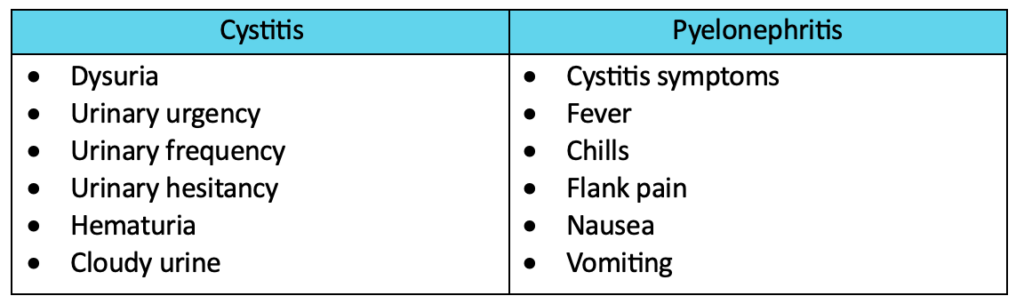
UTI symptoms and diagnosis
Many cystitis symptoms overlap with other urinary tract diagnoses. Likewise, many pyelonephritis symptoms overlap with other types of infections. Therefore, it is important to collect a medical history and a full list of reported symptoms from each patient who presents with a possible UTI.
Diagnosis of UTI is made using a combination of patient-reported symptoms, a detailed medical history, and a urinalysis. No single factor alone should be used to diagnose UTIs.
Treatment for UTIs
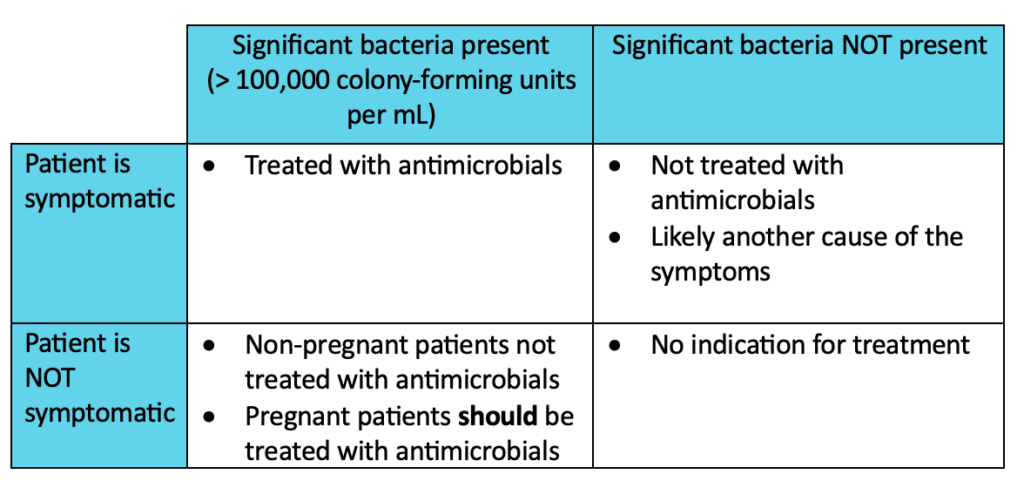
Antimicrobial agents are the main medications used to treat UTIs. However, the agent selected and treatment duration differ between cystitis and pyelonephritis. Medication selection should be patient-specific, taking into consideration previous antimicrobial use, history of UTIs, cost, availability, and allergies. Antimicrobial selection should also be location-specific, taking into consideration local resistance patterns.
Antimicrobial treatment is dependent on the presence of symptoms and significant bacteria in the urine sample. A notable exception is the treatment of pregnant women. All pregnant patients who have significant bacteria present in their urine should be treated with antimicrobials whether they have symptoms or not.
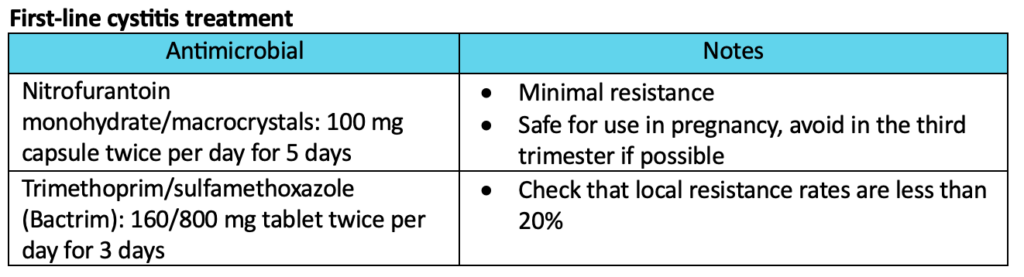
Cystitis treatment:
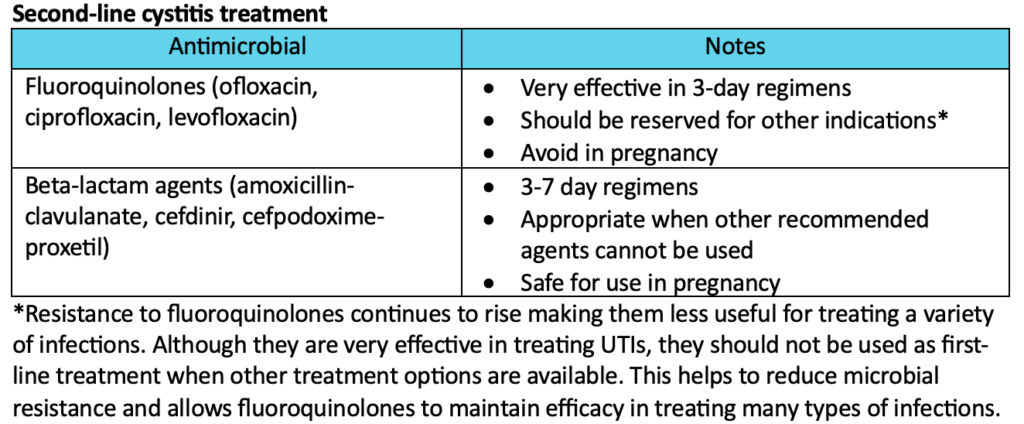
Cystitis treatment generally consists of a short course of oral antibiotics. There are multiple first-line options to choose from, all of which have similar efficacy. Second-line options are reserved for patients who cannot use any of the first-line treatments. Amoxicillin or ampicillin are NOT recommended due to poor efficacy and high resistance.
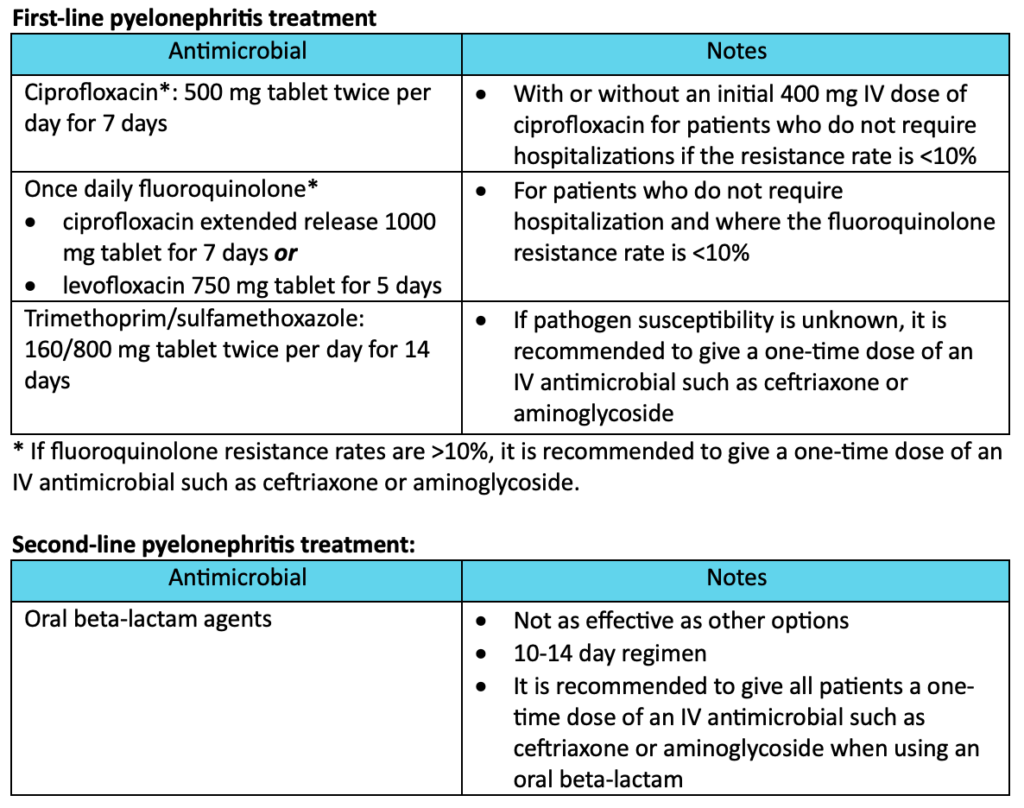
Pyelonephritis treatment
Pyelonephritis treatment generally uses longer courses of oral antimicrobials but may include IV treatment as well. Treatment may take place in the hospital or the outpatient setting depending on the severity of infection. If hospitalization is needed, patients should receive IV antimicrobials initially, then switch to oral treatment. If the patient is treated in the outpatient setting, they may use oral antimicrobials for the full treatment duration. All pregnant patients with pyelonephritis should be treated with IV therapy using ceftriaxone, cefepime, ampicillin plus gentamycin, or aztreonam.
Why is antimicrobial resistance a growing concern?
Antimicrobial resistance occurs when pathogens no longer respond to treatment with specific antimicrobial medications. In these cases, providers are required to prescribe alternative treatments that are not as specific and may come with additional side effects. A study from 2020 found that 1 in 5 UTIs caused by E. coli had reduced susceptibility to first-line treatment options such as trimethoprim/sulfamethoxazole. As more pathogens become resistant to commonly used antimicrobial medications, they will be harder to treat and treatment options will become limited.
Infections that occur due to drug-resistant pathogens have a higher rate of recurrence. It is critical to optimize treatment and limit recurrence by selecting antimicrobials using culture results and local resistance patterns and following guideline recommendations for indication and duration of therapy whenever possible.
What does this mean for pharmacists?
Almost half of the women in the United States will have at least one UTI in their lifetime. This makes UTIs one of the most common problems that require antimicrobial treatment. Pharmacists should consider the treatment guidelines, local resistance rates, and patient-specific factors when making recommendations and verifying prescriptions for UTI treatment.
Pneumonia is a lung infection caused by bacteria, fungi, or viruses. Pneumonia is the leading cause of infection-related death and the 8th most common cause of death worldwide. In the United States, the incidence of community-acquired pneumonia (CAP) is 24.8 cases for every 10,000 adults. Hospital-acquired pneumonia (HAP) occurs in 5-10 of every 1000 hospital admissions, making it the most common infection caused by hospitalization. Antibiotics are the mainstay of pneumonia treatment, and choosing the correct antibiotic depends on various factors. Pharmacists can impact patient care by ensuring that patients receive the most appropriate therapy.
What are CAP and HAP?
Pneumonia is classified by the environment in which the infection occurred and how severe the disease is. Both classifications help to determine treatment options.
CAP is a pneumonia infection that is acquired outside of the hospital. If patients are hospitalized, it is present within the first 48 hours of hospitalization and will show up on initial cultures taken at the time of admission. CAP is the most common type of pneumonia.
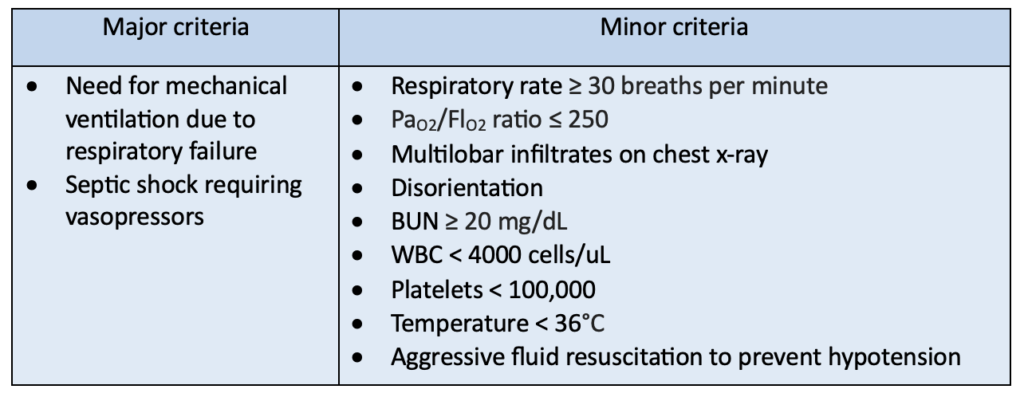
CAP severity is part of the initial patient assessment to determine if a patient should be treated in an inpatient or outpatient setting. Generally, severe CAP is classified as a case with 1 or more major criteria or 3 or more minor criteria.
HAP is a pneumonia infection that is acquired during a hospital stay. It occurs after a patient has been hospitalized for more than 48 hours and is not present on initial cultures upon admission. HAP is less common than CAP but generally requires more robust treatment, which takes place in the hospital.
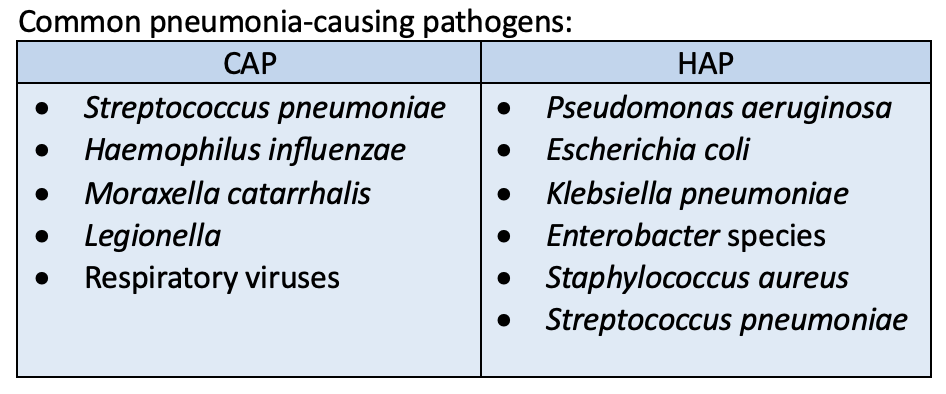
Pathogens that cause CAP and HAP
Pathogens causing pneumonia vary; some pathogens are more common in healthcare settings, while others are more common in everyday environments. Additionally, local infection and resistance patterns for infectious organisms can cause variation in pneumonia pathogens.
What are the signs and symptoms of pneumonia?
Many of the signs and symptoms of pneumonia are consistent with other infections. No single sign or symptom should be used to diagnose pneumonia. Similarly, the lack of a specific sign or symptom should not be used on its own to rule out pneumonia.
Common symptoms of pneumonia include:
Fever
Chills
Chest pain
Cough with sputum production
Shortness of breath
Physical exam and lab findings:
Increased heart rate
Respiratory rate > 20 breaths per minute
Elevated white blood cells (WBC)
Lung crackles or decreased breath sounds
How is pneumonia diagnosed?
Chest X-ray is the gold-standard diagnostic test for patients with suspected pneumonia. The combination of an infiltrate on a chest x-ray and presence of clinical signs and symptoms is indicative of pneumonia and warrants empiric antibiotic treatment.
Respiratory cultures are the main laboratory evaluation used to diagnose pneumonia. However, they can be invasive and easily contaminated. They can be obtained through sputum samples, endotracheal aspiration, and bronchoscopy. Respiratory cultures are not required to diagnose pneumonia and are not commonly performed for patients with non-severe CAP. For patients with more serious infections, including severe CAP and HAP, respiratory cultures can help narrow antibiotic coverage and ensure that uncommon pathogens are appropriately covered by antibiotics.
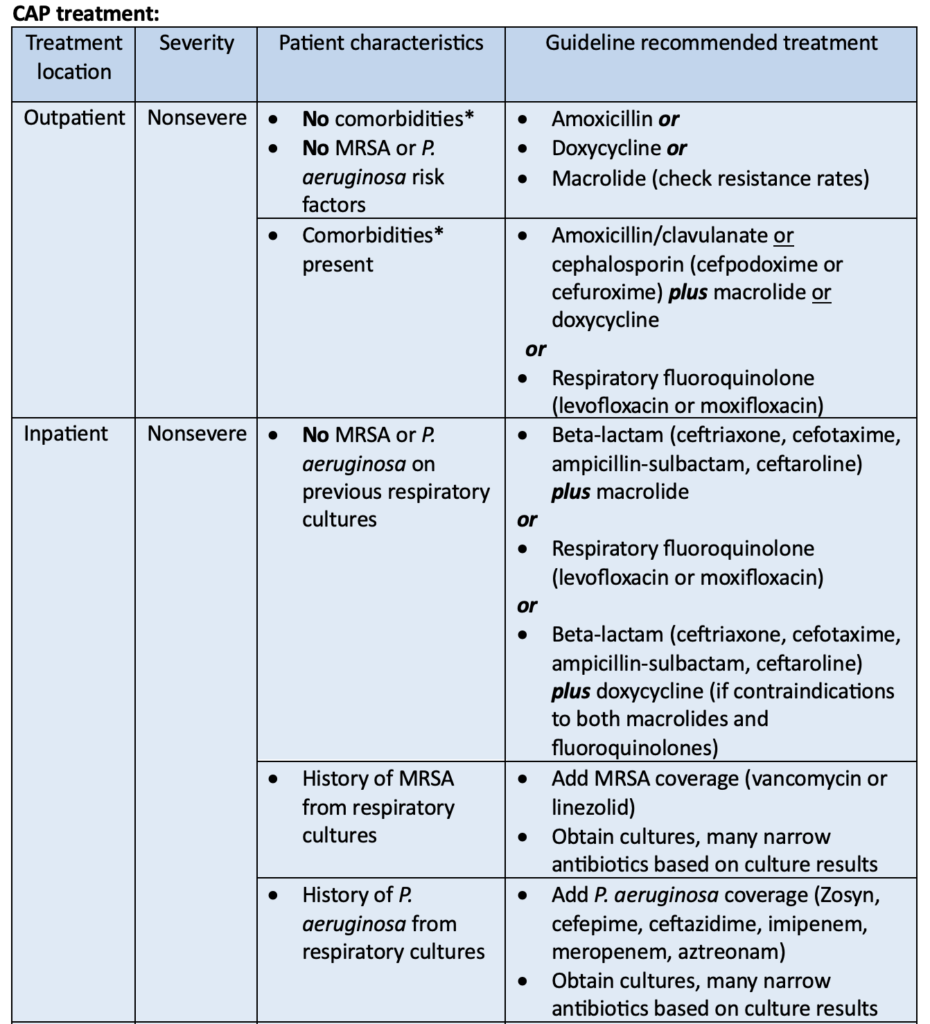
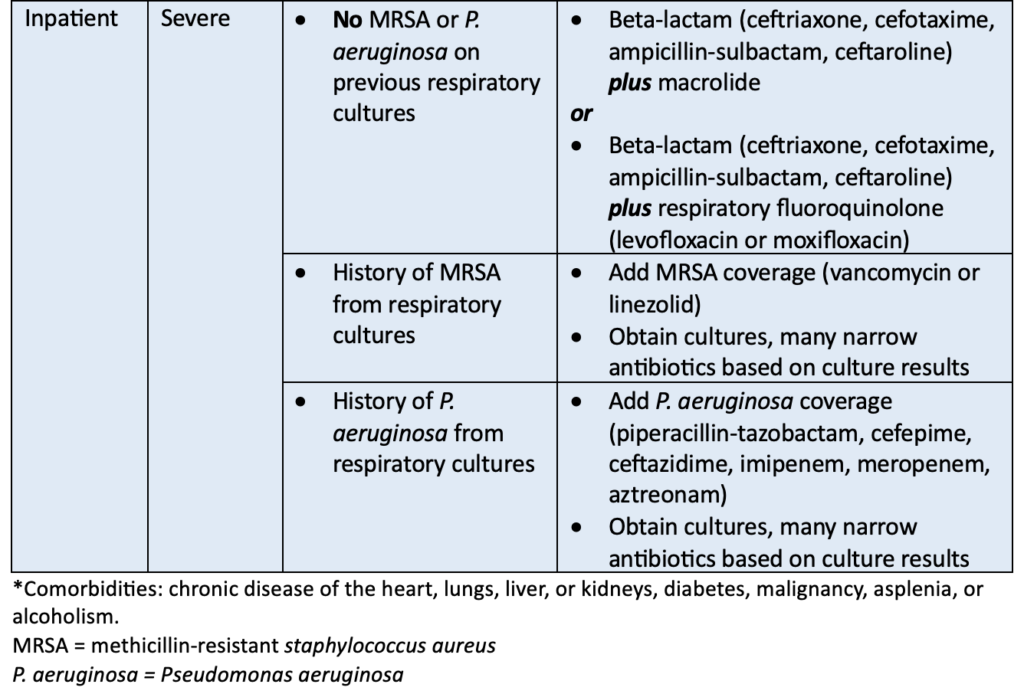
Treatment for CAP and HAP
Antibiotics should be used to treat patients diagnosed with pneumonia. Pneumonia severity, causative pathogen, and local resistance rates should all be taken into consideration when choosing antibiotics from the treatment guidelines. Additionally, patient-specific factors such as allergies, previous infections, and previous antibiotic use should be considered before starting antibiotics.
Treatment for CAP should be continued until the patient is clinically stable and antibiotics have been given for at least 5 days. Clinical stability includes signs that the patient is recovering such as normal heart and respiratory rates, no fever, willingness to eat, stable blood pressure, and normal mental status. The duration of antibiotic treatment may be extended if the patient does not show signs of improvement or the causative pathogen is uncommon and more difficult to treat.
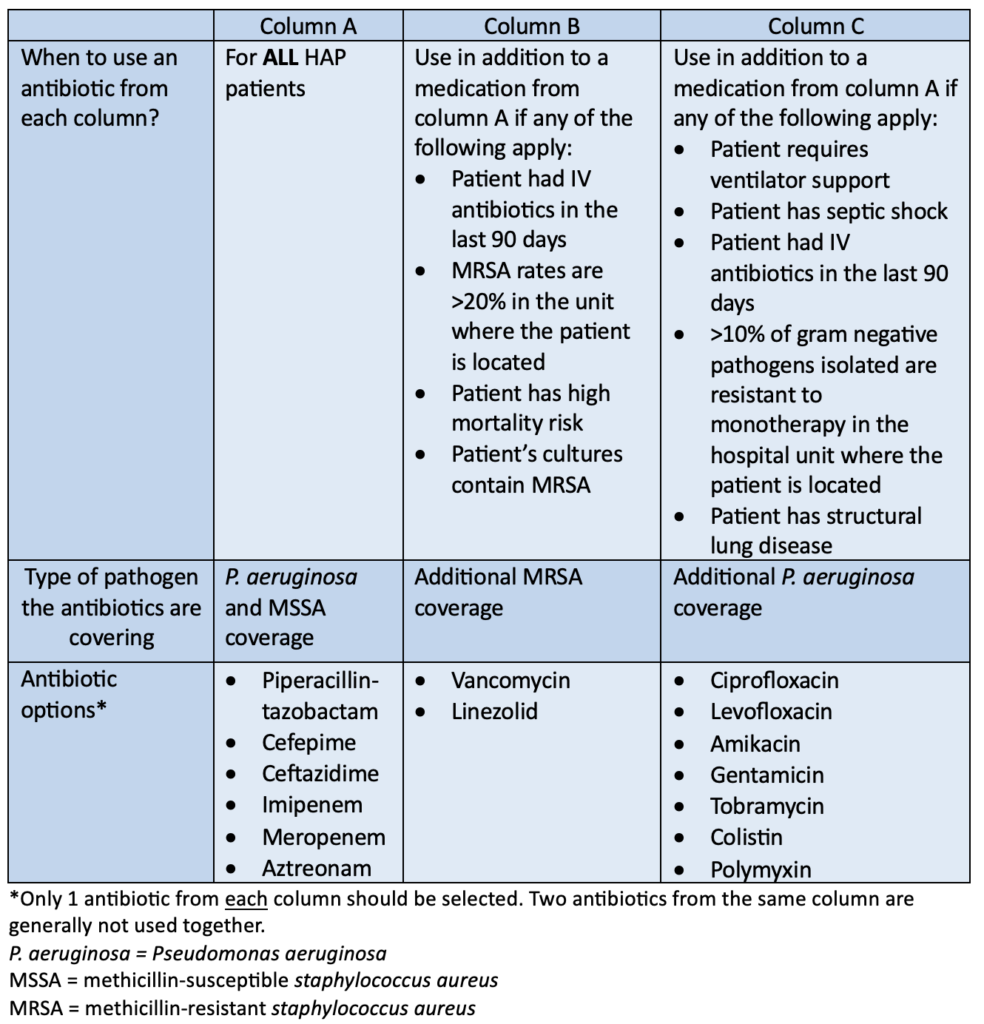
HAP treatment:
All patients who are diagnosed with HAP should be treated with at least 1 antibiotic. This antibiotic should cover P. aeruginosa and methicillin-susceptible staphylococcus aureus (MSSA). Additional MRSA and P. aeruginosa coverage may be indicated for specific patient populations. The table below outlines the guideline-recommended antibiotics for HAP and when additional antibiotic coverage is necessary.
Antibiotics should be narrowed to treat the causative pathogen as soon as possible. Treatment for HAP should be limited to 7 days as long as the patient is clinically improving. Clinical improvement may include a reduction in symptoms, normalized heart and respiratory rates, discontinuation of vasopressors and ventilation, and improved oxygen saturation. Antibiotics may be given for a longer duration if the patient is not clinically improving.
Viral pneumonia treatment
Viral pneumonia is rare and hard to diagnose. The main treatments for viral pneumonia are supportive care and management of precipitating infections.
Supportive care may include:
Supplemental oxygen
Oral or IV fluids
Frequent meals
Rest
Viral infections, such as influenza or respiratory syncytial virus, are the main cause of viral pneumonia. Therefore, giving antiviral medications to treat current viral infections is recommended to help speed up viral pneumonia recovery.
Fungal pneumonia treatment:
Fungal pneumonia is caused by inhaled fungal spores. It is more common in people with weakened immune systems such as organ transplant recipients, cancer patients, and the elderly. Fungal pneumonia is often treated with antifungal medications given either by mouth or IV.
Antifungal medications used:
Itraconazole
Fluconazole
Amphotericin B
How can pharmacists help?
Pneumonia is a common infection caused by a variety of pathogens. It affects a large number of people each year and is classified as community-acquired or hospital-acquired. The main treatment for pneumonia is antibiotics. Pharmacists have in-depth knowledge of antibiotics and should use that knowledge to ensure that patients with pneumonia receive optimal medications to recover promptly.
2016 Clinical Practice Guidelines for the Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia. Infectious Disease Society of America. Available at: https://www.idsociety.org/practice-guideline/hap_vap/. Accessed August 26, 2024.
Heart failure is a complex cardiac disease state that affects more than 6 million people in the United States. In patients with HF, the ability of the heart to eject blood into systemic circulation is decreased due to structural or functional changes that weaken the heart muscle. The approach to treating heart failure includes lifestyle modifications and a combination of medications. New pharmacotherapies continue to be developed and studied for the treatment of heart failure. The PARADIGM-HF trial was a large clinical trial that introduced a new class of medication and ultimately led to a change in the 2022 update of the heart failure treatment guidelines.
What was the PARADIGM-HF trial?
The PARADIGM-HF trial was a randomized, double-blind trial comparing an experimental drug containing sacubitril and valsartan to enalapril, a first-line treatment option, in patients who had heart failure with reduced ejection fraction (HFrEF).
The combination drug studied in this trial is now known by its brand name, Entresto. Entresto is the first drug in a new class called angiotensin receptor/neprilysin inhibitors (ARNi). These medications contain an angiotensin-receptor blocker (ARB) component and a neprilysin inhibitor component. Valsartan is an ARB that is indicated for the treatment of hypertension. It blocks the action of angiotensin II, resulting in less vasoconstriction of blood vessels. Sacubitril is a neprilysin inhibitor that blocks the breakdown of vasoactive peptides, such as bradykinin. This counteracts vasoconstriction and cardiac remodeling.
Previous studies showed that using ARBs and neprilysin inhibitors together was more beneficial than utilizing either medication on its own in heart failure treatment. Studies also found safety concerns with an increased risk of angioedema when studying angiotensin-converting-enzyme (ACE) inhibitors in combination with neprilysin inhibitors. Therefore, they were not used together in this study or in practice.
When this trial was published in 2014, ACE inhibitors were an essential treatment option for patients with HFrEF, because they had been shown to reduce mortality. ARBs showed lack of evidence for mortality reduction and were only recommended for use in patients who could not tolerate ACE inhibitors.
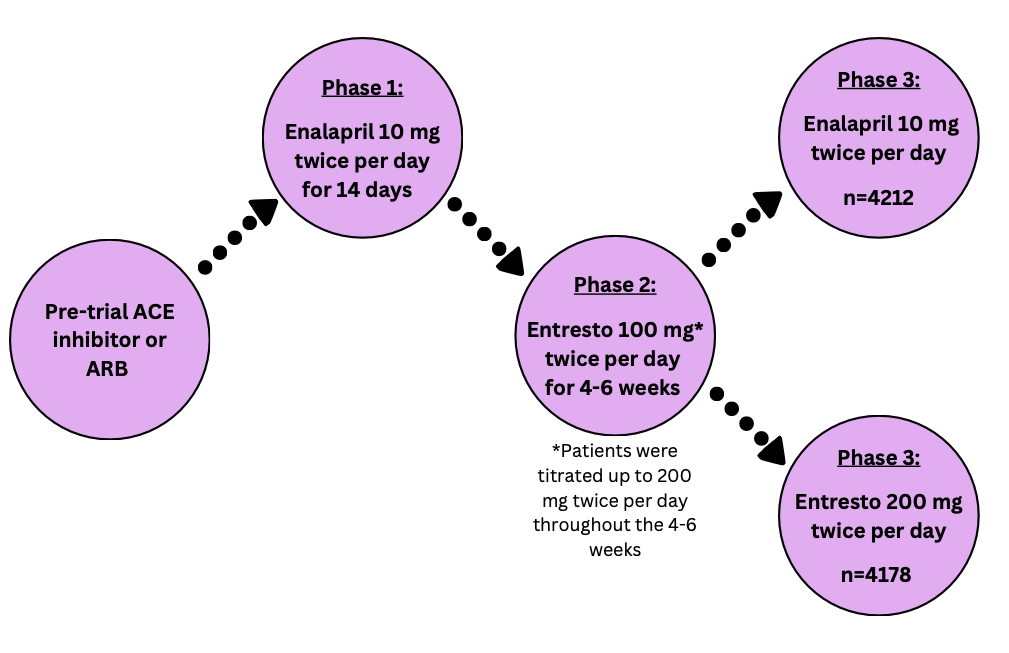
How was the study conducted?
The PARADIGM-HF trial had three main phases. After phase one and two, patients who could not tolerate the medication were removed from the study. The intention-to-treat population was analyzed with a total of 8399 patients split into the two treatment groups.
Image created with Canva
Patients enrolled in this study had moderate to severe disease and tolerated medication to treat heart failure. Patients excluded from this study had conditions that made it unsafe to take the treatment medications.
Notable* inclusion criteria:
New York Heart Association Class II, III, or IV heart failure
Ejection fraction of 35% or less
Pre-study ACE inhibitor or ARB dose equivalent to 10 mg of enalapril or more
Stable use of a beta blocker and ACE inhibitor or ARB for at least 4 weeks
Notable exclusion criteria:
Hypotension, defined as a systolic blood pressure of <100 mmHg
Previous angioedema or serious side effects to ACE inhibitors or ARBs
(*This list is not exhaustive and includes the highlights for patient enrollment parameters)
Many of the primary and secondary endpoints are reflective of common events that happen in patients with heart failure due to their decreased cardiac function.
The primary endpoint measured was a composite of:
death from any cardiovascular cause
heart failure symptoms causing hospitalization for the first time
Multiple secondary endpoints were measured including:
Time from treatment to death from any cause
Change in the Kansas City Cardiomyopathy Questionnaire (KCCQ) from baseline to 8 months
New atrial fibrillation onset
Renal function decline
During statistical analysis, the intention-to-treat population was analyzed using Cox’s proportional hazards model. Hazard ratios (HR) and confidence intervals (CI) were reported.
Outcomes of the trial
The PARADIGM-HF trial was stopped early due to overwhelming evidence that Entresto showed superior benefit.
The primary endpoint occurred in 21.8% of patients treated with Entresto and 26.5% of patients treated with enalapril. This outcome was statistically significant with a p-value <0.001, favoring the use of Entresto over enalapril.
All primary endpoint components were individually evaluated and found to be statistically significant in favor of Entresto. The secondary endpoints of death from any cause and changes from baseline in KCCQ scores were also statistically significant in favor of Entresto. The remaining secondary endpoints showed no significant differences between the two treatment groups.
The most common side effect reported for Entresto was hypotension. For enalapril, common side effects included cough, hyperkalemia, and decreases in eGFR. Overall, 10.7% of patients taking Entresto and 12.3% of patients taking enalapril stopped taking the medication due to side effects.
Entresto, a combination drug consisting of sacubitril and valsartan, was more effective than enalapril alone at reducing mortality from cardiovascular causes or hospitalizations due to heart failure for patients with HFrEF. The safety profiles of these two medications were similar with enalapril having a wider variety of reported side effects.
What does this mean for pharmacists?
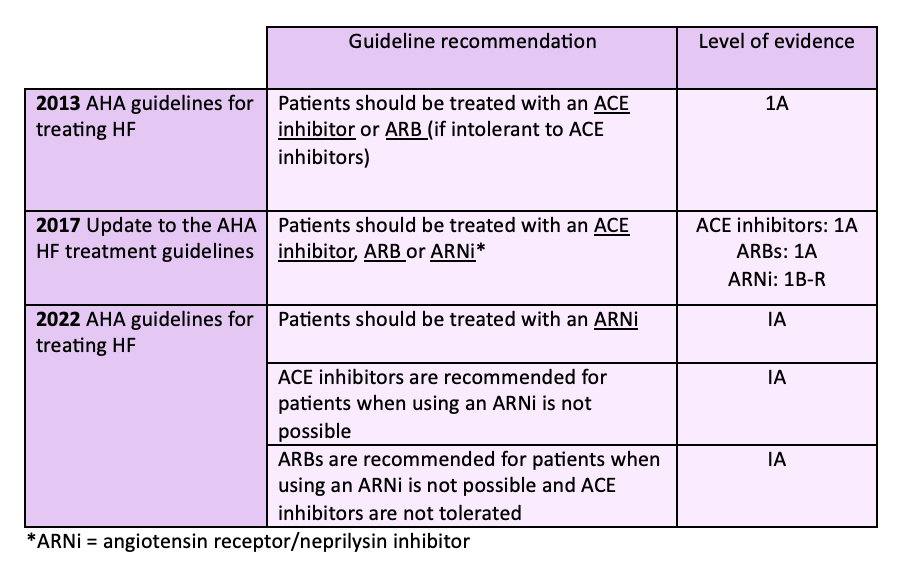
The heart failure treatment guidelines have evolved over the last 10 years as data from the PARADIGM-HF trial and other landmark HF trials has been published. The table below shows the progression of the guidelines for treating patients with HFrEF.
It is now recommended to use an ARNi for HFrEF treatment unless there are factors prohibiting its use. ACE inhibitors and ARBs are still safe and effective choices for treating patients especially those who may not be able to afford a brand name-only medication such as Entresto.
As pharmacists, it is important to stay up to date on landmark trials and the effect they have on treatment guidelines. The PARADIGM-HF trial showed less mortality and fewer hospitalizations for patients with HFrEF when using an ARNi compared to an ACE inhibitor. The outcome of this trial led to changes in the treatment guidelines for HFrEF to include a new class of medications that provide stronger benefits for patients.
Margaret M., APPE Student
References:
Angiotensin-Neprilysin Inhibition versus Enalapril in Heart Failure. The New England Journal of Medicine. 2014;371:993-1004. DOI: 10.1056/NEJMoa1409077. Available at: https://www.nejm.org/doi/full/10.1056/NEJMoa1409077. Accessed August 21, 2024.
2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Available at: https://pubmed.ncbi.nlm.nih.gov/23747642/. Accessed August 21, 2024.
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Available at: https://www.ahajournals.org/doi/10.1161/CIR.0000000000000509. Accessed August 21, 2024.
2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Available at: https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001063. Accessed August 21, 2024.
Pharmaceutical compounding is an important part of the care that pharmacy staff provide for patients daily. The United States Pharmacopeia (USP) sets national standards for nonsterile and sterile pharmacy compounding in USP <795> and USP <797> respectively. These standards outline the information needed to compound a safe pharmaceutical product, from training requirements to personal garbing, to beyond-use dates, and more. On November 1, 2022, USP issued major updates to USP <795> and USP <797>. Pharmacies around the country had until November 1, 2023, to put these changes into practice. As a pharmacist, it is important to understand and implement the most updated USP guidelines to ensure the accuracy and safety of all the products the pharmacy generates. Reviewing these major changes will also be critical for pharmacists studying for licensure!
Why where USP <795> and <797> changed?
USP <795> and <797> were updated for the following reasons:
To reflect improvement in pharmacy practice and science
To provide clarification on information that was commonly misunderstood
To integrate ideas from stakeholders
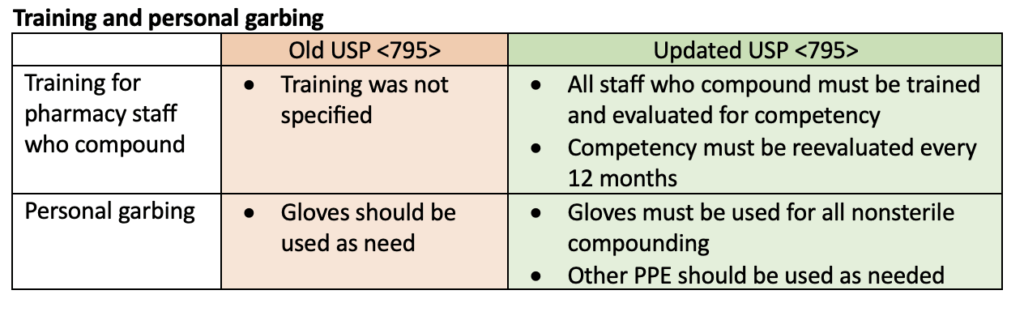
Updates to USP <795> for nonsterile pharmacy compounding
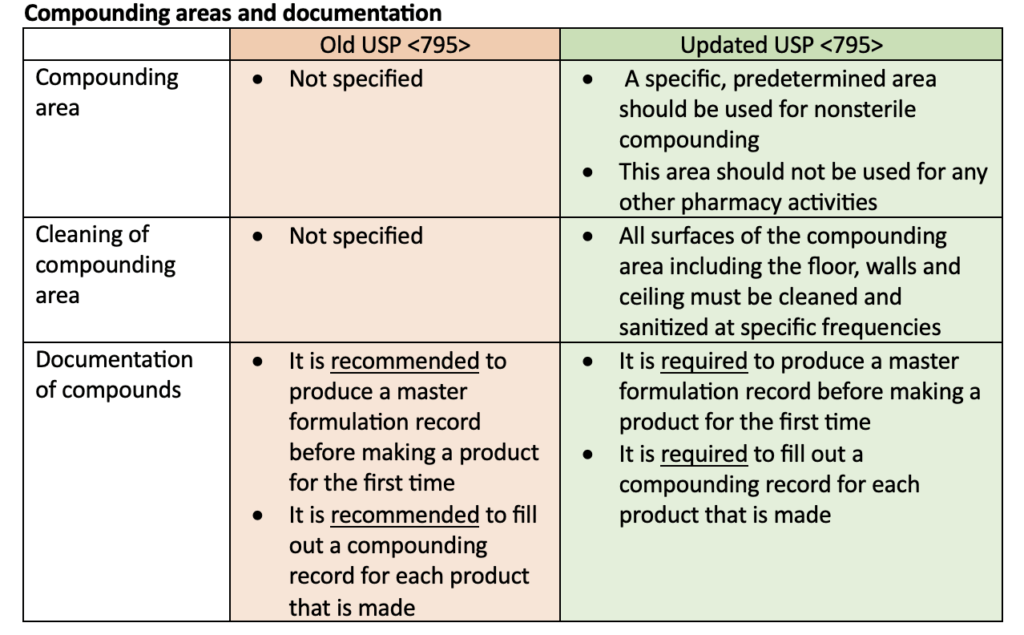
Multiple updates were made to USP <795> including training and personal garbing requirements, specifications for compounding areas, instructions for using master formulation and compounding records, and changes to beyond-use dates (BUDs). The following tables highlight some of the updates to the USP <795> requirements.
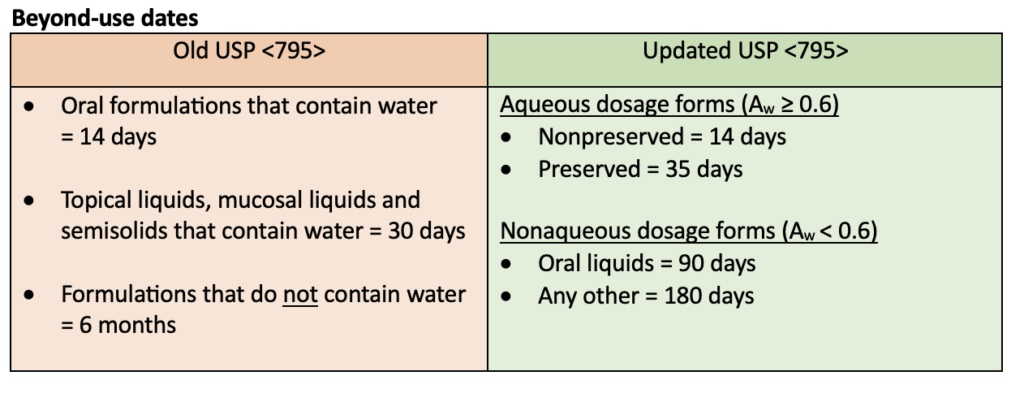
BUDs were the biggest change when USP <795> was updated in 2022. Nonsterile compounds are now defined by their water activity instead of being categorized as nonaqueous or water-containing. Water activity (Aw) is used to determine how likely contamination by microbes and/or degradation by hydrolysis is to occur for nonsterile compounded products. Aqueous products have an Aw ≥ 0.6 and nonaqueous products have an Aw < 0.6.
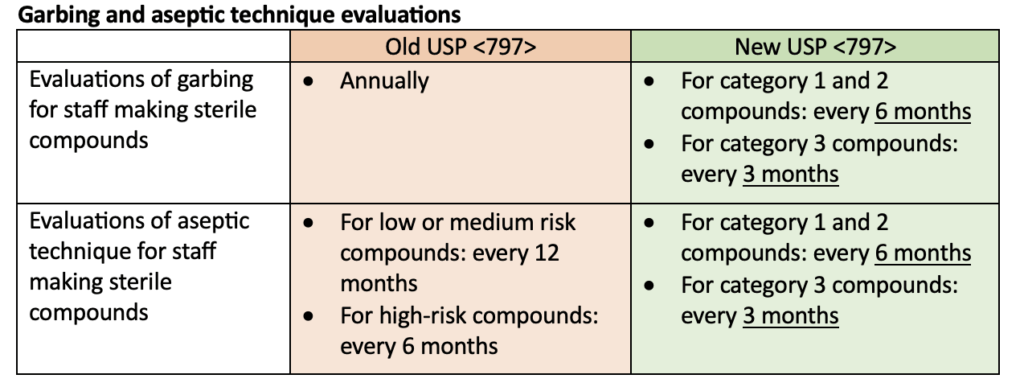
Updates to USP <797> for sterile pharmacy compounding
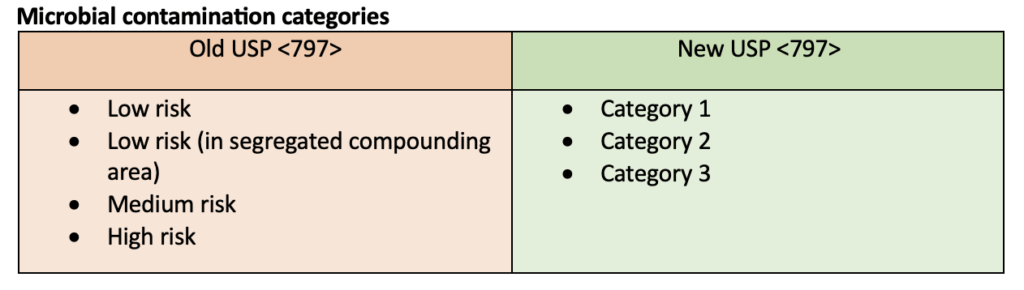
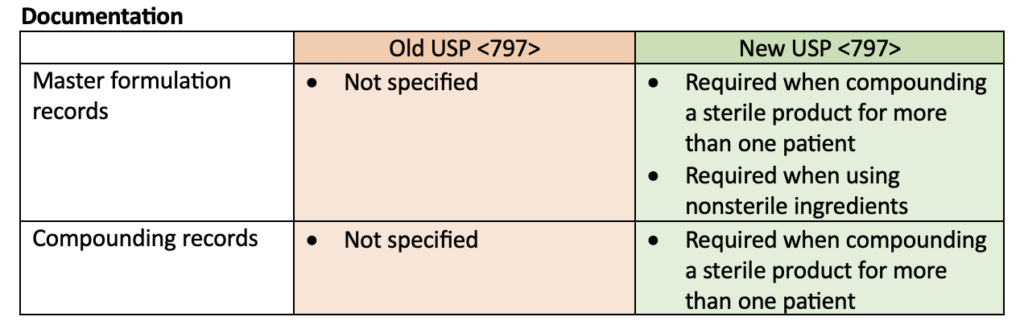
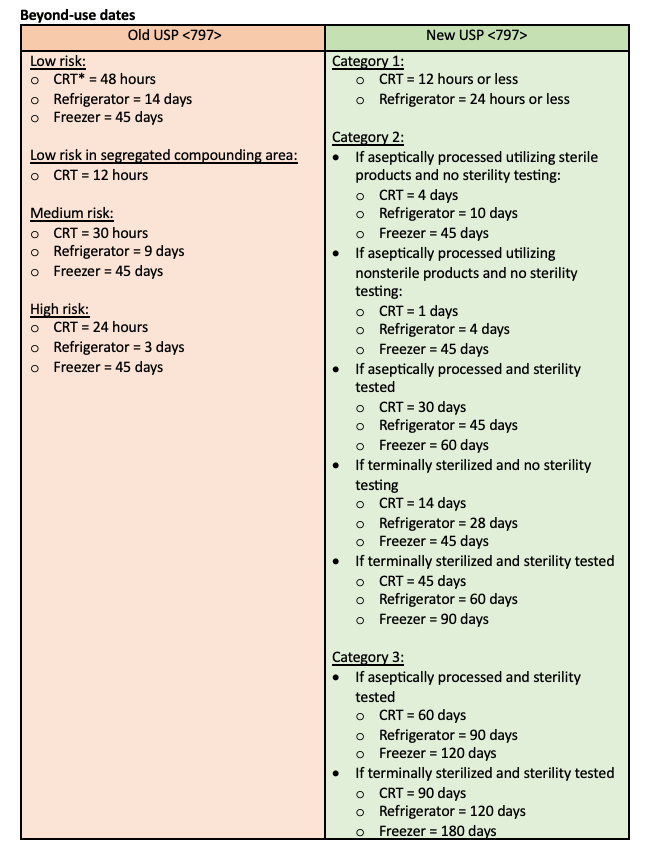
Many updates were made to USP <797>. The most notable update was a change in the definition of microbial contamination categories for sterile compounded products. This definition change was reflected in many of the other updates including personal garbing, aseptic technique evaluations, and beyond-use dates. Requirements for master formulation records and compounding recorders were also specified. The following tables compare the old USP <797> requirements to the new USP <797> requirements but do not represent all the changes made.
Category 1 compounds must be prepared in at least an ISO Class 5 area that is placed in a segregated compounding area. These compounds require the least amount of environmental control.
Category 2 compounds must be prepared in a cleanroom and require more control of the environment than category 1 compounds.
Category 3 compounds must be prepared in a cleanroom. They undergo additional sterility testing and have added requirements for the area in which they are compounded so that they can have longer BUDs. Those requirements include additional training, sterile garb, cleaning, and monitoring of the environment.
*CRT = controlled room temperature
Putting these changes into practice!
USP <795> and <797> have recently been updated to improve standards of practice in compounding. These changes encompass a wide variety of updates from personal garbing to beyond-use dates. It is important to implement and follow these new guidelines in every pharmacy that provides compounding services for the health and safety of all patients.
The FDA recently approved the first over-the-counter (OTC) birth control pill, Opill. Opill’s active pharmaceutical ingredient was previously approved as a prescription-only medication. Still, given the absence of prescriber oversight, pharmacists must be especially prepared to counsel and answer questions about this medication.
What is the new OTC birth control?
Opill is a daily progestin-only pill (POP) that can be used to prevent pregnancy. It is the first and only oral birth control pill to be available over the counter. Opill is very similar to other POPs in both ingredients and mechanism of action. The main difference between Opill and other POPs is that Opill does not require an appointment with a provider or a prescription. It can be purchased at many drugstores and online.
About Opill
The active pharmaceutical ingredient in Opill is 0.075mg of norgestrel.
Opill’s mechanism of action is the same as other POPs. It works by:
Causing the cervical mucus to thicken
Slowing ovulation
Lowering the LH and FSH peaks
Image created with Canva
The most common side effects of Opill and other POPs are:
Irregular, breakthrough bleeding between periods
Headaches
Weight gain and/or increased appetite
Nausea
Abdominal cramping
Cost: A 28-day supply of Opill costs $19.99.
When to use POPs such as Opill
A benefit of POPs is that they do not contain estrogen. This makes them a favorable option for patients who want to take an oral contraceptive but have a contraindication to estrogen-containing products such as combined hormone contraceptives (CHCs).
Contraindications to CHCs include:
Hypertension that is not controlled
Smoking more than 15 cigarettes per day (if the patient is over 35 years old)
Migraines with aura
History of stroke
History of venous thromboembolism
Breast cancer or history of breast cancer
Endometrial cancer
Valvular heart disease
ASCVD
Liver cirrhosis
Diabetes with microvascular complications
One of the main risks of CHCs is venous thromboembolism (VTE) due to the estrogen component of the medication. Estrogen increases blood coagulability which increases the patient’s risk of VTE. Since POPs do not contain estrogen, they do not present the same clotting risk and are safer for OTC use.
When not to use POPs such as Opill
It is also important to understand when POPs are contraindicated and should not be used.
POP contraindications include:
Uterine bleeding that is atypical and undiagnosed
Breast cancer or a history of breast cancer
Previous bariatric surgeries
Liver cirrhosis
Coadministration with certain medications to treat seizures, HIV, or tuberculosis
Important counseling points
Most norethindrone-based POPs, such as Opill, do not have any placebo tablets. Therefore, it is critical that patients do not skip any of the tablets.
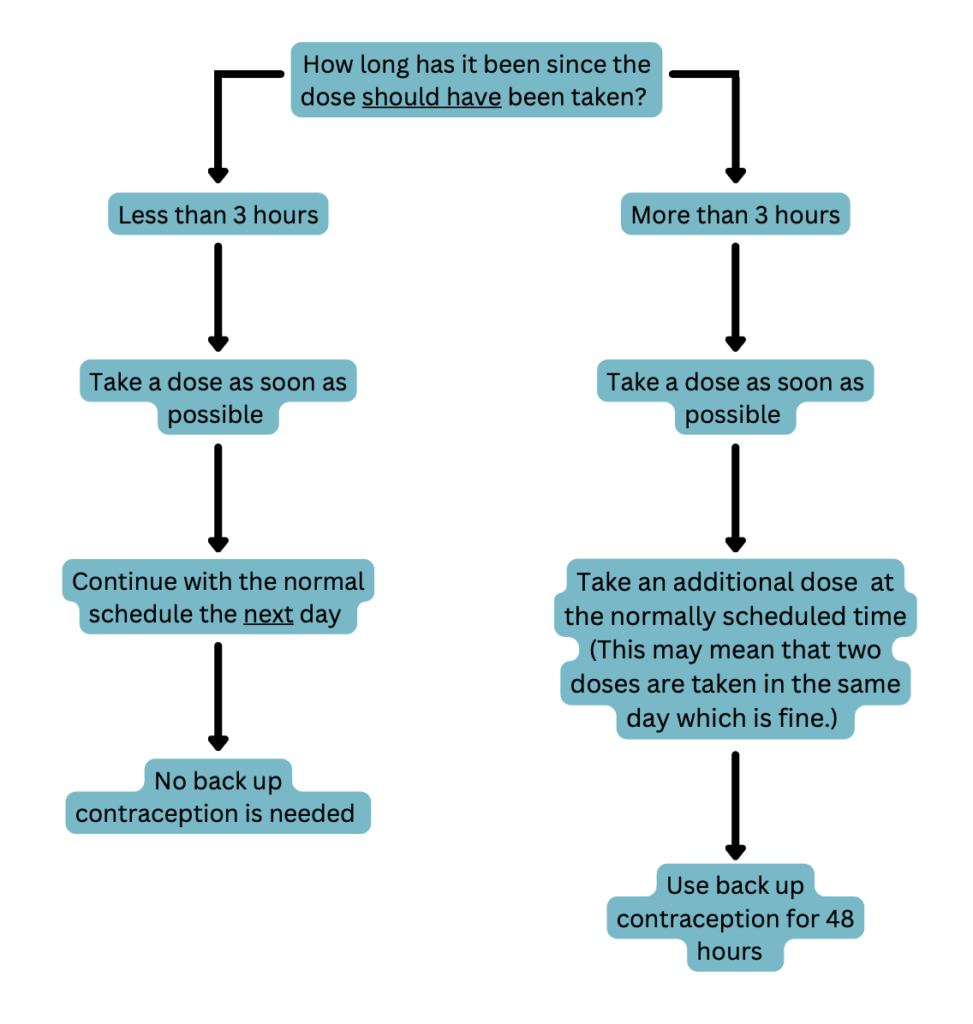
POPs are very time-sensitive due to their short half-lives of about 8 hours. Thus, it is important to remind patients to take their tablet at the same time each day to keep their contraceptive concentrations consistent. Encourage them to set a reminder on their phone or take this medication at the same time as another daily activity such as eating breakfast or dinner. If an individual misses a dose they should proceed in 1 of 2 ways depending on how many hours they are past the time they normally take the tablet. See the following flowchart for details.
Image created with Canva
Patients should see a medical provider if they develop pain in their lower abdomen, migraines with aura, or jaundice while taking POPs. They should also see a medical provider if they become pregnant or develop intolerable side effects.
An additional form of contraception, such as condoms, should be used for 48 hours after starting POPs and any time a patient is 3 or more hours late taking a dose. Other forms of hormonal birth control should not be used as backup contraception for POPs.
Birth control pills, including POPs and CHCs, are about 93% effective making them more effective than barrier methods (87% effective) but less effective than implants such as IUDs (99% effective). Like most birth control, the effectiveness of POPs is directly dependent on the individual’s ability to take the medication as directed. This means taking the medication at the same time each day and never missing a dose.
Because the effectiveness of birth control pills is directly related to medication adherence, pharmacists need to discuss all birth control options with patients to help them decide if an OTC option is best or if they should see a provider for a prescription-only option. OTC birth control pills may not be the best choice for everyone. For example, someone who is unable to adhere to a strict dosing schedule may require a prescription-only alternative, such as an implant. On the other hand, OTC birth control pills may be a great option for people who have limited access to healthcare providers and may not be able to get a prescription.
What does this mean for pharmacists?
Opill, the new over-the-counter birth control pill, was recently FDA-approved and is now being sold in many drug stores. This medication is very similar to prescription POPs with the biggest difference being its OTC status. Neither an appointment with a prescriber, nor a prescription is necessary to start taking Opill. This provides an accessible option for patients who have limited access to healthcare providers. Although increased accessibility is important, birth control pills do come with risks and contraindications. Pharmacists need to be ready to have risk versus benefit discussions about all birth control options and help patients choose the option that is best for them. Pharmacists should also be prepared to counsel and answer questions about Opill, because they are likely to be the main healthcare providers advising patients who are considering this medication.
Migraine is a complex disease state that presents most commonly with headaches that are often severe and can be accompanied by environmental sensitivity, nausea, or vomiting. About 12% of the population is affected by migraines, and they are caused by controllable and uncontrollable triggers. The pathophysiology of migraine is not clearly defined. However, there are many treatment options available to treat migraines acutely and prevent future migraine attacks.
What is a migraine?
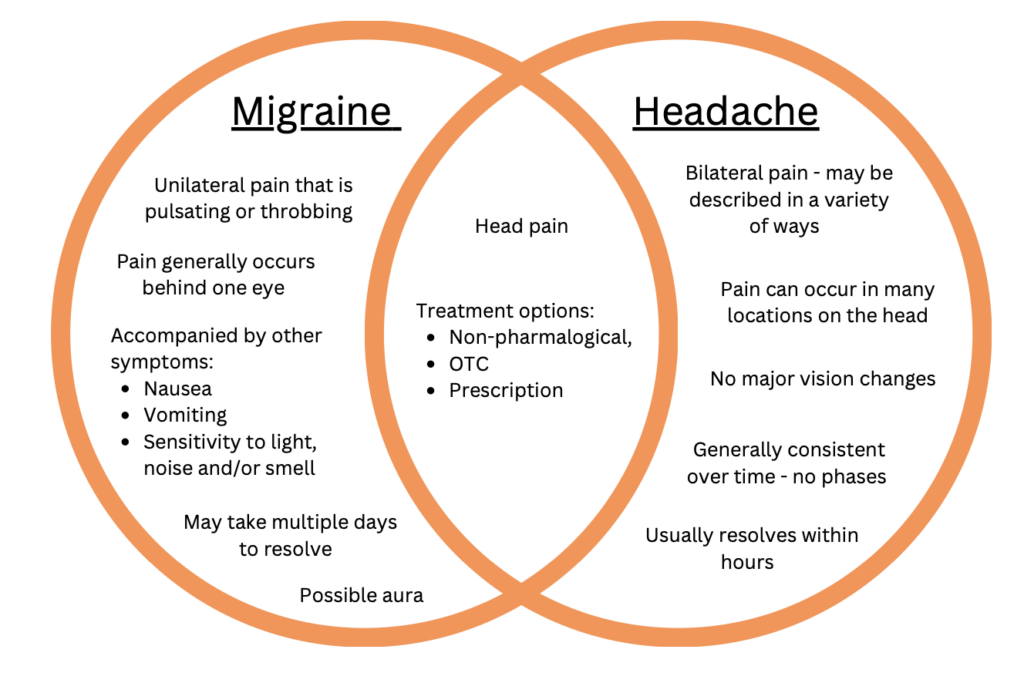
A migraine is a headache that is moderate to severe and recurring over time. Migraines are characterized by one-sided head pain and are often accompanied by nausea, vomiting, and heightened sensitivity to light, noise, and smell. The duration can range from a couple of hours to three or more days.
Image created with Canva
The two most common types of migraines are migraine with aura and migraine without aura. They share many characteristics, such as one-sided head pain, nausea, vomiting, and sensitivity to light, noise, and smell. The main difference between these two types is the presence or absence of aura. Aura is a reversible sensory disruption with symptoms such as blind spots, blurry or flashing vision, or tingling of the face. It occurs directly preceding or concurrently with a migraine. These symptoms are present in migraines with aura and absent in migraines without aura.
Migraines are also classified by how often they occur:
Chronic migraine is defined as 15 or more headache days per month, with at least eight of the headaches having symptoms of migraine, for at least three months.
Episodic migraine is any migraine that does not occur frequently enough to be considered chronic.
Who gets migraines?
People worldwide are affected by migraines, although they are most common in North America.
Image created with Canva
They happen more frequently in the following populations:
Women – it is 3 times more likely for women than men
Anyone with a family history of migraines – migraines have a genetic component and most people who suffer from migraines also have a family history of migraines.
Migraines commonly start at the onset of puberty and continue to occur well into adulthood. However, they can affect people of any age. Generally, migraines become less frequent later in life, especially after menopause in women.
Migraine triggers
Migraines can be caused by both predictable and unpredictable triggers which are patient-specific. Additionally, an unpredictable trigger for one person may be a predictable trigger for another person.
Predictable triggers may include:
Hormonal changes — such as throughout a menstrual cycle
Stress – migraines often occur after a period of prolonged stress
Unpredictable triggers may include:
Changes in sleep
Alcohol
Smoking
Head injury
Changes in environment – loud noises, strong smells, bright lights
Missed meals or low blood sugar
Migraine pathophysiology
The pathophysiology of migraine is not well understood. One theory involves the activation of the trigeminal nerve and the subsequent release of neuropeptides, which cause vascular vasodilation within the meninges. Vascular vasodilation contributes to inflammation of neurons, which causes pain. Two of the neuropeptides that have a role in this pathway are serotonin and calcitonin gene-related peptide (CGRP). These neuropeptides are targets in some of the pharmacologic treatment options.
The four phases of migraine
Prodrome – occurs up to 24 hours before migraine due to activation of the hypothalamus.
Symptoms include frequent yawning, change in mood, hunger, edema, and increased fatigue.
Aura – occurs due to fluctuations in cortical function and circulation of blood. It can last minutes to hours and happens before or during the headache phase.
Symptoms may include blind spots, blurry or flashing vision, or tingling of the face.
Aura is present in about 35% of migraines.
Headache – occurs for hours to days due to changes in the activity of many parts of the brain including the thalamus, brainstem, hypothalamus, and cortex.
Other symptoms include nausea, vomiting, and heightened sensitivity to light, noise, and smell.
The hallmark symptom is pulsing or throbbing head pain that occurs on one side of the head.
Postdrome – occurs hours to days after the headache has ended.
Common symptoms include fatigue and dizziness.
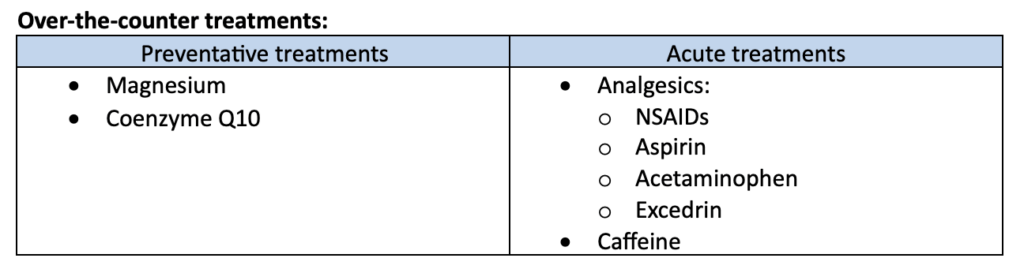
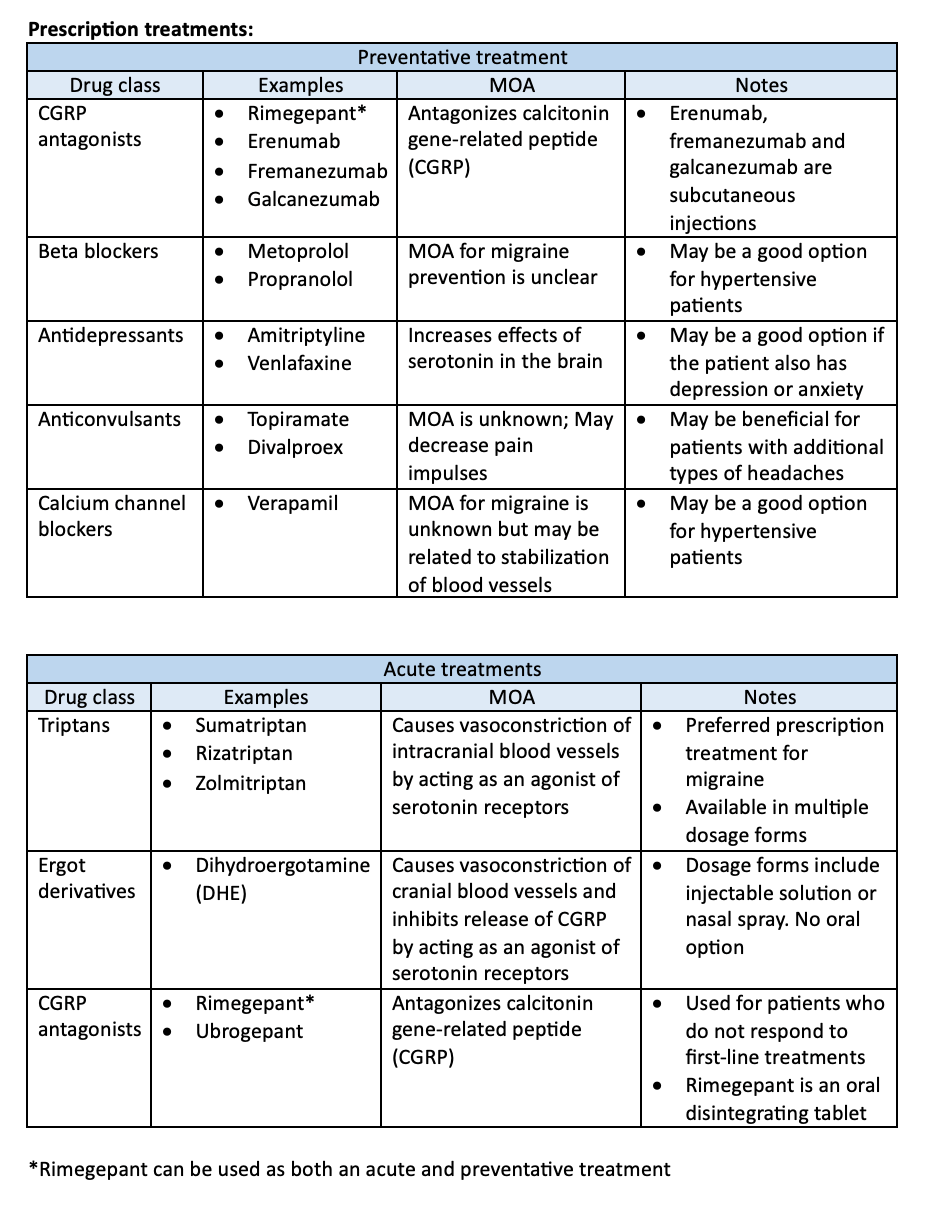
Migraine treatment
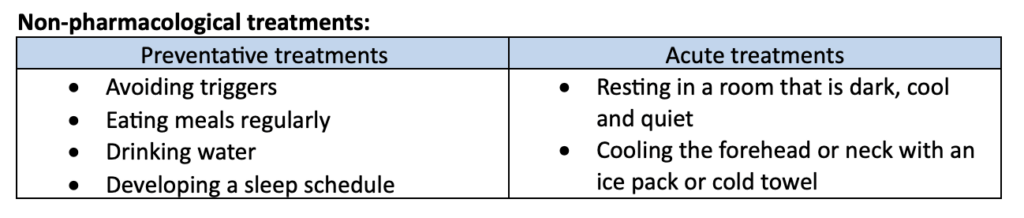
Treatment goals include stopping current migraine symptoms and avoiding future migraine episodes. There are many non-pharmacological, over-the-counter, and prescription treatment options for migraines. All treatment strategies can be classified as acute or preventative treatment.
Acute treatment is used as needed to stop current migraine symptoms. Preventative treatment is used consistently to prevent future migraines from occurring. Treatment strategies are patient-specific and may include a combination of prescription and non-prescription treatments. Additionally, patients can use acute and preventative treatments individually or in combination.
Migraine is a neurologic disease with episodes caused by a variety of triggers. Generally, migraines last hours to days while cycling through 4 phases and should be treated with patient-specific approaches. Luckily, there are many treatment options, including non-pharmacological, over-the-counter, and prescription therapies. Migraines can be treated acutely as they occur or with a preventative treatment strategy. It is important to understand common migraine triggers and the multitude of treatment options to best educate and treat patients with migraine.