My path to success began with unfathomable pressure and consequently, failure. Remember – if at first you do not succeed, try, try again.
After failing my NAPLEX twice I reached out to one of my former professors from pharmacy school for advice. I needed new study material and support to try again. Having recently being introduced to RxPharmacist, she recommended I email them to see if they could help. I reached out as suggested and after one phone call with the founder of RxPharmacist I had been offered the opportunity to write a study guide for my upcoming AL MPJE and receive study help for my next attempt at passing the NAPLEX.
I was given access to professional medical writers that could guide me through writing the Alabama Pharmacy Law Review and a practice exam to go with it. My preceptor/editor helped me learn the ins and outs of medical writing and editing. I felt the steep learning curve, but I worked hard and got the job done. My editor and the founder supported me throughout the writing process, and I learned the best way to write a guide and the questions necessary for the practice exam. After completing the guide and the practice exam, I got to build the online course. With my love for informatics, building the online course was my favorite part of this experience.
As part of this opportunity, I have also been part of the RxPharmacist “How to Get a Job” series where the founder teaches how to network effectively, craft your resume, compose your cover letter, prepare for an interview, and negotiate salary once you receive the job offer. This information has been invaluable to me, and I cannot thank RxPharmacist enough for allowing me to be a part of this educational series.
I have been given access to law and NAPLEX study materials, instructed in the intricacies of medical writing and editing, and the nuances of getting a job. With support of RxPharmacist behind me and the confidence to do what needs to be done I can get my license and my dream job.
The path to success has many turns and speed bumps, but with the right support and self-confidence you will reach your destination.
During a career pivot I found myself in need of guidance and support. It was during this uncertain time that RxPharmacist emerged as a great mentorship opportunity, offering invaluable assistance that not only honed my writing skills but also influenced my professional journey. Their commitment to my growth was evident throughout my entire internship. RxPharmacist provided unwavering support and guidance, serving as a mentor during this pivotal stage of my career. During my internship I was encouraged to think outside the box and explore creative approaches to creating medical education. This resulted in new points of view, new thought processes, and unique learning opportunities outside of the traditional learning methods. RxPharmacist not only recognized my potential as a medical writer but also challenged me to push the boundaries of my capabilities, resulting in projects that were both impactful and engaging. These realizations transcended the projects completed, positively impacting my engagement with both clinical and industry connections and opportunities. I appreciated the autonomy they gave me during my projects while always being available for questions. This benefited my skills to work independently, as well as with a team, applying feedback and collaborating on the most efficient ways to complete objective. RxPharmacist expected accuracy and precision throughout my time with them and their emphasis on thorough research and meticulous editing elevated my writing skills. This standard ensured that every piece of content was the highest quality and integrity.
As I navigated the ups and downs of my career and personal life, RxPharmacist was a constant source of support and encouragement. Their mentorship extended beyond professional guidance, encompassing personal development and well-being. Throughout the internship, I gained invaluable knowledge that has benefited my objectives through my career pivot, as well as the connections I have since made through unique networking channels. I will definitely continue to use, and benefit from, the skills, lessons, and connections I have made through the RxPharmacist internship. Whether I needed advice on navigating career challenges or simply a listening ear, RxPharmacist was always there, offering advice and unwavering support. As I look back on my journey with RxPharmacist, I am filled with gratitude for the invaluable lessons learned and the profound impact it has had on my career and personal growth. Thanks to their mentorship and support, I feel confident and empowered to take on new challenges and explore opportunities for growth. To anyone embarking on a career in pharmacy, I wholeheartedly recommend RxPharmacist as a guiding group to help you on your path to personal and professional success.
The support, learning, and unquantifiable benefits of the RxPharmacist internship will prove to be instrumental in my success getting through this unique period in my life. Although my situation may be untraditional, I believe the resources and opportunities of RxPharmacist would be beneficial to fellow pharmacists in various stages of their career. Whether you are in college, recently graduated, or have experience but would like to change paths, RxPharmacist would be an excellent option for maximizing your career potential.
-Spring 2024 RxPharmacist Intern, Lipscomb University
I was initially captivated by RxPharmacist from the moment I heard about the prospect of participating in an online internship tailored to my interests. The flexibility to set my pace and customize assignments aligned perfectly with my preferences. RxPharmacist not only acknowledged my interests but went above and beyond, providing enriching work experiences that would resonate in my future endeavors.
Throughout the internship, the unwavering support from RxPharmacist was a cornerstone of my success. The ability to articulate my gained experiences during interviews was a testament to the valuable projects I undertook. Focused on my passion for advertising and promotion, I had the opportunity to engage in projects that not only aligned with my interests but also expanded my horizons into the realm of medical writing.
Becoming an editor for the GA MPJE guide was a crowning achievement, allowing me to contribute significantly to a project of great importance. The mentorship and guidance I received from RxPharmacist Preceptors played a pivotal role in refining my skills and broadening my perspective. The comprehensive learning experience fostered growth, making each task a stepping stone toward professional development.
Thanks to the Preceptor’s support, I was sponsored by this internship to attend ASHP MidYear and I was able to secure a coveted fellowship position at Rutgers, precisely in the area I aspired to be. This accomplishment was a direct result of the skills honed during my internship, showcasing the tangible impact RxPharmacist had on my career trajectory.
In retrospect, RxPharmacist not only met but exceeded my expectations. The internship was not just a learning opportunity; it was a transformative experience that propelled me into a position I had only dreamed of. The symbiotic relationship between my interests, the assignments tailored by RxPharmacist, and the mentorship I received culminated in a success story that I proudly carry into my professional life.
In conclusion, RxPharmacist is not merely a platform for internships; it’s a catalyst for growth, a facilitator of dreams, and a bridge to unparalleled opportunities. I am immensely grateful for the pivotal role RxPharmacist played in shaping my career, and I wholeheartedly recommend it to anyone seeking an internship experience that goes beyond expectations.
I recently completed an internship with RxPharmacist, having learned about the opportunity through my school newsletter. I am writing to express my sincere gratitude for the enriching experience and to provide feedback on the valuable insights gained during my time as an intern.
Prior to joining RxPharmacist, I had completed a rotation with a pharmaceutical company in the scientific communications division. It was during this period that I discovered my keen interest in medical writing. Eager to further develop my skills, I applied for the RxPharmacist internship and was thrilled to be accepted.
Throughout my internship, I had the opportunity to work on editing MPJE guides for three different states. Each guide presented a unique set of challenges as they were formatted differently, and the process of understanding and consolidating pharmacy laws from diverse sources proved to be a valuable learning experience. I discovered that not all states provide straightforward access to their laws online. Some require additional effort to compile and update the necessary information for the guides. RxPharmacist MPJE guides combine information from all sources in one document for the purpose of assisting users with simplifying their studying process and ensuring they pass their exams from the first try.
One of the most commendable aspects of the internship was the continuous and detailed feedback I received from my preceptor. Their insights were instrumental in enhancing my medical writing and punctuation skills. I appreciated the accessibility of the preceptors, who could be contacted at any time via Slack and were prompt in responding to queries. The one-on-one sessions offered allowed me to clarify instructions and address any confusion. Interns are fully supported by their preceptors who are always available to answer any questions or confusions.
The feedback received after each project draft proved invaluable, helping me identify and rectify errors I was previously unaware of. I learned various techniques on Microsoft Word to maintain consistent formatting and avoid common pitfalls. I honed my paraphrasing skills while simplifying complex pharmacy laws by properly referencing laws and ensuring accurate representation.
Additionally, the internship provided an opportunity to enhance my question creation skills, a task assigned to generate a specific number of questions for each guide. This not only improved my understanding of the content but also contributed to my preparation for the MPJE exam. Looking at the laws of different states through this internship also raised my awareness on similarities and differences of pharmacist scope of practice in different states which can restrict a pharmacist in one state while permit in another.
Other than the projects, this internship also offers free ‘How to find a job’ live sessions during the fall (as well as for summer internship programs) where students can learn proper resume or CV presentation, how to answer interview questions, how to negotiate salaries, and much more. The instructor is available in the session to ask questions, discuss concerns, and practice elevator pitch and interview questions. This program has helped several students find jobs upon graduation and I am excited to use the skills I learned to find a job once I graduate.
Despite the challenges of managing the internship alongside school commitments during the fall semester, I appreciate the understanding and flexibility demonstrated by my preceptor when extensions were necessary. I wholeheartedly recommend this internship to anyone seeking to improve their medical writing skills.
Thank you once again for the invaluable experience, and I look forward to applying the skills acquired during my time at RxPharmacist in my future endeavors.
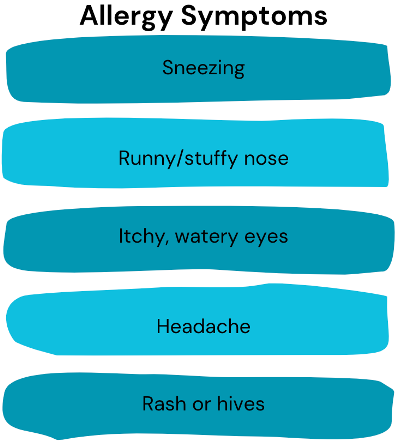
Picture this: you see someone. They’re sneezing. Their nose is runny. Their eyes seem to be watery, and they keep rubbing them like they’re itchy. If you thought to yourself, “That person could use a hanky”, well you’re probably not wrong. But if you also thought, “Looks like they have allergies”, then you nailed it. Some people have had allergies for as long as they can remember. Some may not have ever had allergies then they moved someplace else and suddenly developed them. Others might be lucky enough to never develop them in the first place. The truth is that pesky allergies exist in many forms and arise from multiple allergens. We’ll investigate the why, what, and how when it comes to allergies.
Allergies occur because of the body’s immune system and its overreaction to a certain substance that it deems as an ‘intruder’ or ‘harmful’. This results in an allergic reaction. Any substance that causes such a reaction is labeled an ‘allergen’. Usually these allergens are relatively harmless, and what may trigger a reaction in one person may not cause the same reaction in another.
There are different kinds of allergies triggered by various allergens: food, pet, latex, mold, and drug, to name a few. Allergic rhinitis or ‘hay fever’ is used to describe the condition causing the symptoms previously described such as sneezing, runny nose, and itchy, watery eyes. Allergies may be seasonal or perennial meaning that it doesn’t just occur depending on the season but rather year-round. It is usually triggered by pollen. While sneezing and itching are milder and more common symptoms of an allergic reaction, hives and anaphylaxis are more severe symptoms that require prompt medical care.
Allergy Testing
It is important to figure out what triggers an allergy as sometimes the triggers may not be obvious. If allergies are suspected, an allergist would be the best healthcare provider to go to. Their roles involve performing allergy testing, identifying the trigger, and accurately diagnosing the condition. After a complete medical history and physical exam is done, an allergy test may be performed. Common allergy tests include:
● Skin testing – a tiny drop of allergen is pricked onto the skin or injected underneath ● Blood testing – involves a single needle prick and a sample is sent to a lab ● Patch testing – the allergen is applied to a patch which is then applied to the skin
Management and Treatment
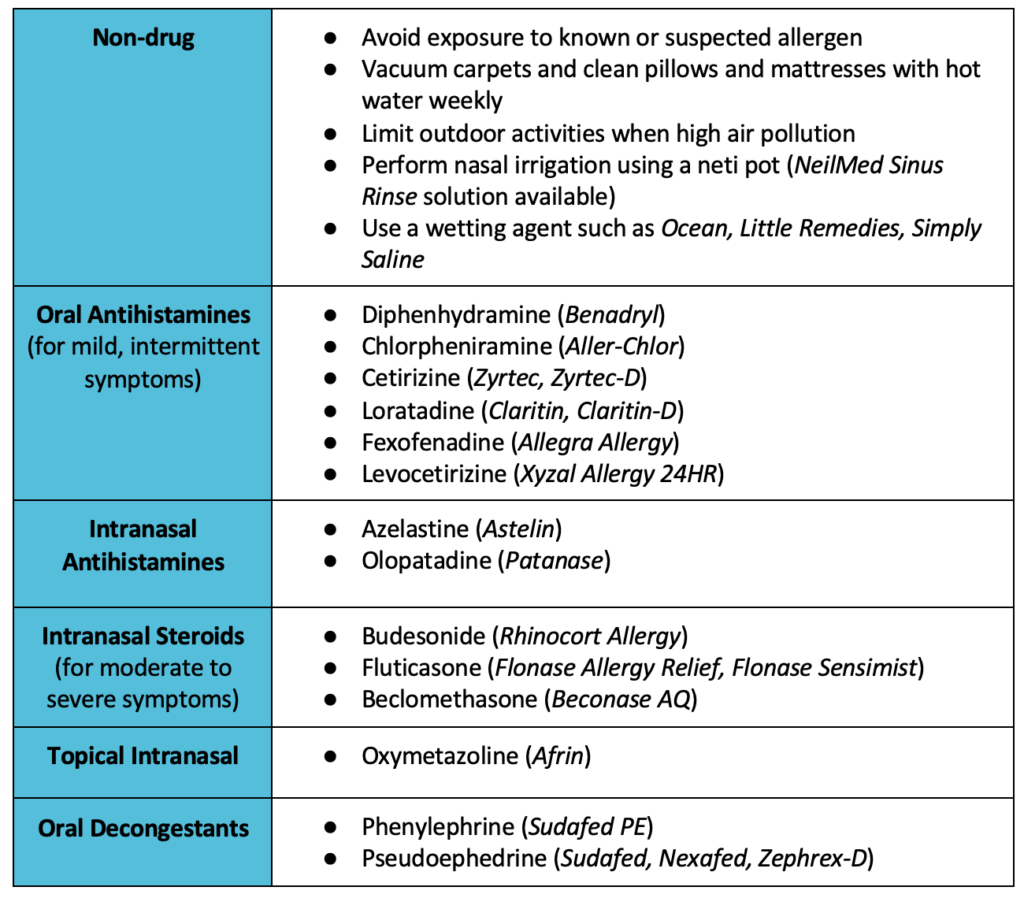
If triggers are obvious and able to be anticipated, most patients can be treated completely with over the counter (OTC) medications. Some may still need prescriptions to alleviate their allergies. Regardless, pharmacists are in an important position for helping patients select the appropriate OTC options to help manage their symptoms. Pharmacists can help patients acquire the right oral antihistamine, decongestant, intranasal steroid, or eye drop based on the symptoms present. Patients should always consult with a doctor or pharmacist before taking any OTC drug. Some common treatment options for allergies include the following:
Allergies can be a nuisance, but dealing with them shouldn’t have to be. By understanding why they occur and recognizing the common triggers, patients can make informed decisions on what action to take to treat their condition as quickly as possible. In addition, patients can also come to recognize who to seek out for help (such as pharmacists) in selecting the most effective treatment option that is available.
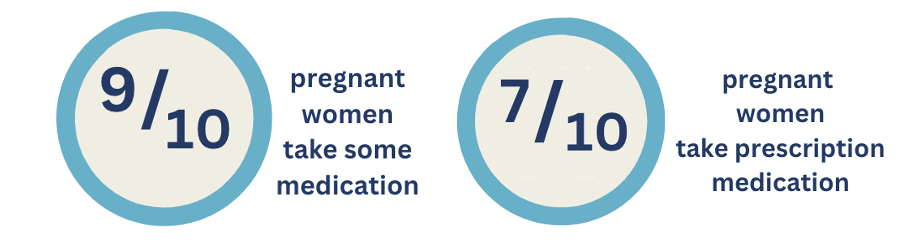
Are you taking medication? Are you pregnant? Are you pregnant AND taking medication? These are important questions to consider especially for women of childbearing age as medication use during pregnancy is quite common. Per the CDC, 9 out of 10 women take some type of medication with 7 out of 10 women taking at least one prescription medication.1
Women who are pregnant and/or lactating experience major physiological and psychological changes that require special attention to medication and healthcare. Pharmacists are in a unique position to offer additional advice in terms of medication safety, nutritional support, and general well-being in managing acute pregnancy issues. Not only does this ensure that the mother is provided with the safest and utmost care possible, but that the health of the baby is considered in equal measure as well.
Medication Safety
For all children and adults, it is important to speak to a doctor prior to using any medication, whether it’s a prescription drug or an over the counter (OTC) drug. During pregnancy and lactation, this warning is ever more critical to remember.
Taking inappropriate medication without proper consultation with a doctor may cause some undesirable effects in certain adults who are yet otherwise healthy. Women who are pregnant and/or lactating however, are more vulnerable for experiencing harm from certain kinds of medications, as is the baby.
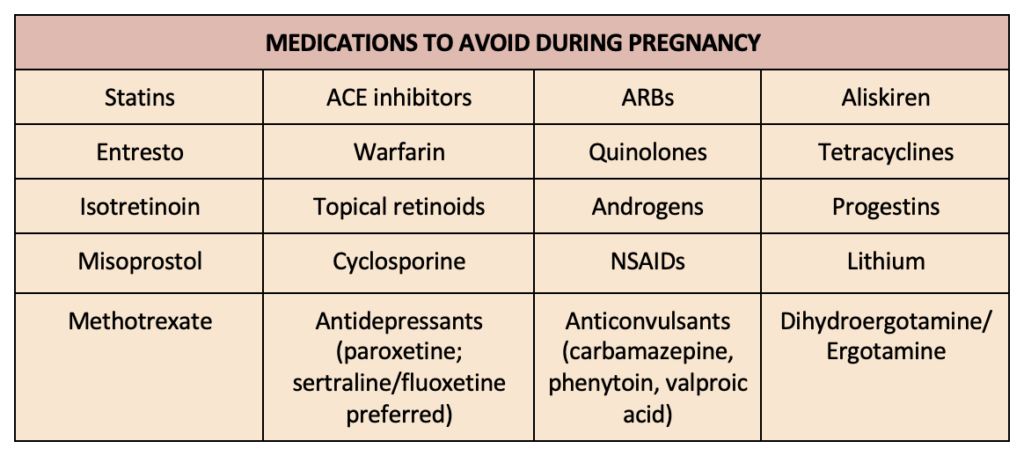
Drugs that are considered toxic to the developing fetus during pregnancy (i.e., result in birth defects) are known as teratogenic drugs, and pose the most risk during the first trimester. Some medications may also decrease milk production during lactation. These drugs should be discontinued before pregnancy or once a woman is determined to be pregnant and safer options should be utilized instead.
Nutritional Support- Vitamin and Mineral Supplementation
A developing baby needs an appropriate amount of nutrients. Two vital examples of important nutritional support are folic acid and calcium and vitamin D. Deficiencies in folic acid (i.e., folate) causes birth defects of the brain and spinal cord known as neural tube defects, whereas deficiencies in calcium and vitamin D can hinder the development of the skeletal system.
Folic acid: Foods rich in folic acid include green leafy vegetables, dried beans, cereals, and orange juice. The recommended dietary folate equivalent (DFE) per day is 600 mcg DFE per day during pregnancy.
Calcium and Vitamin D: During pregnancy, 1000 mg per day of calcium and 600 IU per day of vitamin D are recommended. This can either be achieved through supplements or natural sources. Some foods rich in calcium include milk, cheese, yogurt, and green leafy vegetables.6 Good natural sources for Vitamin D include sunlight, milk, and fish/salmon.6
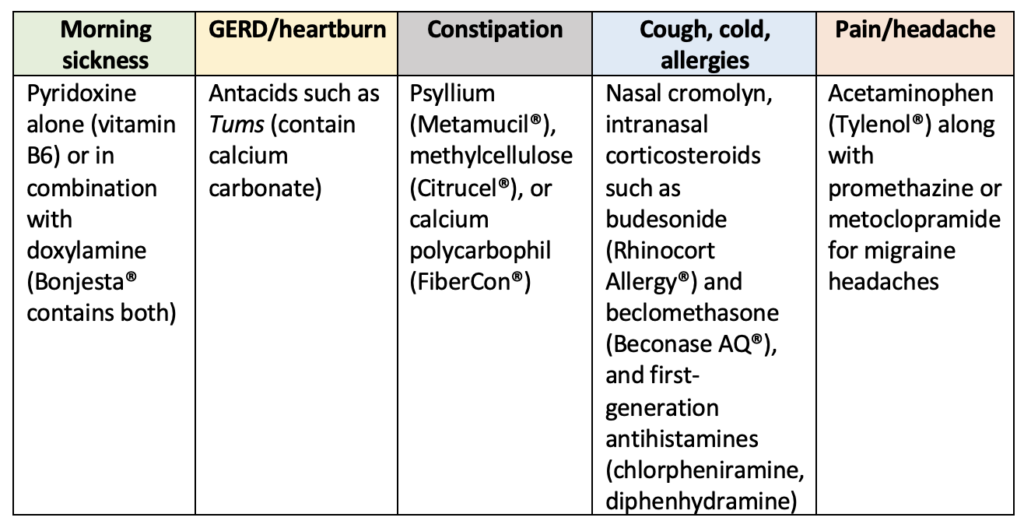
Common Pregnancy Discomforts and How to Treat Them
While not an all-inclusive list of all issues experienced during pregnancy, below are some drug treatments for common discomforts. Lifestyle measures or behavioral interventions will always be first line before implementation of drug therapy. These include eating smaller, more frequent meals while avoiding spicy food for morning sickness and GERD/heartburn. Drinking more water and increasing physical activity helps with constipation. Using hot/cold packs and relaxation/stress management techniques are useful in managing pain and headaches.
Enrolling in a pregnancy registry is also encouraged to help gather information on the use of a drug during pregnancy. For each woman, the journey will be unique, therefore personalized guidance from healthcare professionals remains paramount. Through collaboration and consultation with healthcare providers, making informed choices about medications and supplements, and focusing on proper nutrition, women can embrace pregnancy with confidence and optimal health. Some helpful resources for additional information are:
Currently, in a rapidly evolving healthcare landscape, the world of medicine relies heavily upon facts and evidence. As a healthcare professional, making informed decisions about medications, treatments, and interventions is crucial. What role does evidence-based medicine (EBM) play into all of this? Let’s investigate.
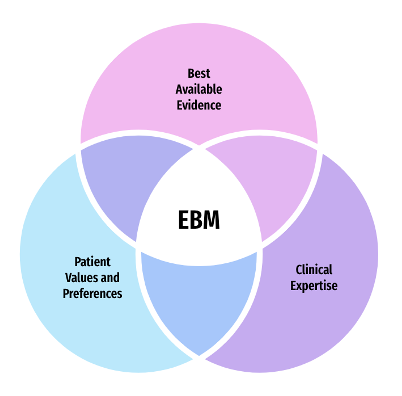
As a pioneer in EBM, Dr. David Sackett’s most recent definition of it is: “The integration of best available evidence with clinical expertise and patient values into the decision-making process for patient care.”1 EBM serves to provide a scientific framework for being able to ask and provide answers to clinical questions while keeping in mind the needs of the patient in different clinical settings. The components of EBM fall into three categories: best available evidence, clinical expertise, and the values and preferences of the patient.
(Best Available) Evidence: refers to the findings from clinical research, from the best available resource that is relevant to patient care.2 These findings can be from systematic reviews, and clinical research from experimental and observational studies. It is the gathering of research information to help inform decision-making.
Clinical Expertise: involves using clinical skills and experience to evaluate evidence related to the patient’s current health status.2 Pharmacists have the skills and experience related to pharmacotherapy and clinical service. They can be valuable resources in both the access and translational aspects of pharmacotherapy evidence as this is relevant to patient care.
Patient Values and Preferences: refer to the goals, expectations, and beliefs that patients have for decisions and their outcomes.2 The values and preferences of a patient regarding the healthcare choices they make or decide upon are based on their beliefs, attitudes, cultural, and spiritual factors. It is vital to ensure that delivery of healthcare is mindful of all these factors and that they are used as a guide when it comes to clinical decisions.
Another way to view EBM is to look at it as a course of action: you receive a question, you search for the data to help answer the question, and then you end your search by relaying the information found. This course of action, in fact, can also be outlined in the 4 steps below.2
Step 1: Ask an Appropriate and Answerable Clinical Question ○ Make sure it is properly structured and guides the evidence search ○ What is the focus of the question? What type of information are you looking for? Step 2: Find the Evidence ○ Search published literature from relevant resources ○ PubMed or Cochrane Library Step 3: Appraise the Evidence Found ○ Review relevant information (all evidence ≠ each other) along with internal validity ○ Per the “Hierarchy of Evidence”, systematic reviews/meta-analyses are ranked the highest, then randomized controlled trials, and then cohort studies Step 4: Apply the Evidence to Practice ○ External validity – can the results be applied to other populations, or more specifically, the patient in question? ○ Determine if the evidence is clinically significant, statistically significant, neither, or both
Through these steps, EBM incorporates interventions that work based on the high quality of evidence found, helps encourage communication among healthcare professionals, and facilitates the skill of research and keeping up with new information. However, that is not to say it is without its challenges or limitations. Individual patient factors must always be considered which may not always be synonymous with the evidence found, nor does EBM focus on explaining how the interventions are likely to work.
Making informed decisions in improving pharmacotherapy care is most effective through the utilization of EBM. Appropriate knowledge and skill are necessary to get the most out of it. EBM’s role in healthcare is inarguable, and it will continue to make an impact for years to come.
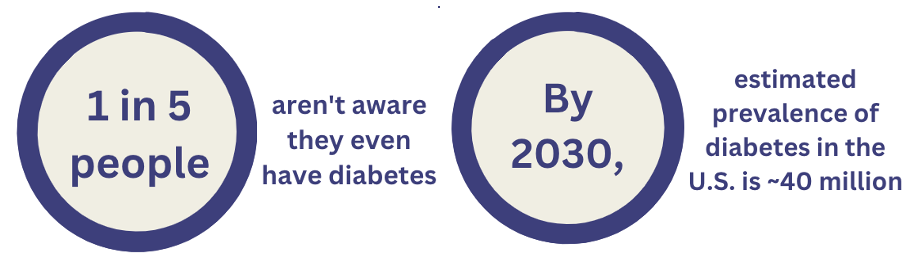
Diabetes as a health condition has become so prevalent that the number of cases are reported to be the highest that they have ever been. Per CDC, ~37 million people in the United States have diabetes and 1 in 5 people don’t even know that they have diabetes.1 Moreover, prevalence, is projected to continue to rise in the coming years reaching almost 40 million by 2030.6
That doesn’t mean it’s all doom and gloom. Diabetes can be managed with medication treatment, and even better, prevented or delayed with achievable lifestyle changes. But there are different kinds of diabetes, and despite the name, they’re not all the same nor are they treated in the same manner. Here we’ll focus on type 1 and type 2 diabetes, what makes them different, their symptoms, and their management.
Overview of Diabetes
Diabetes mellitus (DM) is a chronic health condition where your blood glucose, or blood sugar, is too high. Insulin is a hormone produced by the pancreas that helps to control blood glucose by allowing glucose to enter cells and provide the body with energy. By affecting insulin, the blood glucose is also affected. The body is relying on its star player in this role to keep blood glucose in check. Without insulin, blood glucose will rise, leading to health problems over time with key organs such as the heart, kidneys, eyes, and nerves being damaged. There is no cure for diabetes.
Type 1 vs Type 2
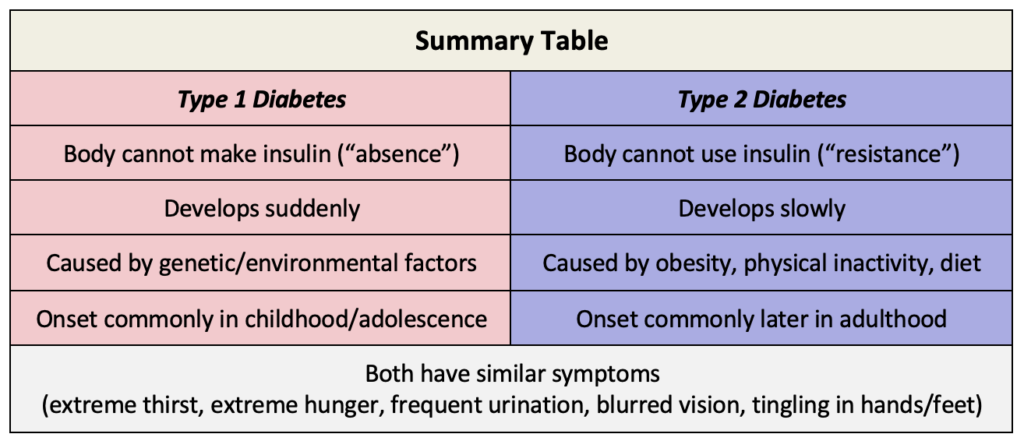
Both type 1 diabetes mellitus (T1DM) and type 2 diabetes mellitus (T2DM) have some sort of malfunction issue with insulin, causing it to become deficient.
In T1DM, the body cannot make insulin, stops making it, or it is not making enough of it because the cells in the pancreas that produce insulin are destroyed by the body’s own immune system. The primary cause is believed to be caused by genes and/or environmental causes. It can develop in early childhood/adolescence compared to later in adulthood in people with T2DM.
In T2DM, the body cannot use the insulin despite still making it. Insulin resistance is usually the primary cause of T2DM due to physical inactivity and obesity. Because of this resistance, the body is less able to absorb glucose over time which is why this condition is slow progressing. This contrasts with T1DM where the body is not able to absorb glucose at all and the condition can develop quite suddenly.
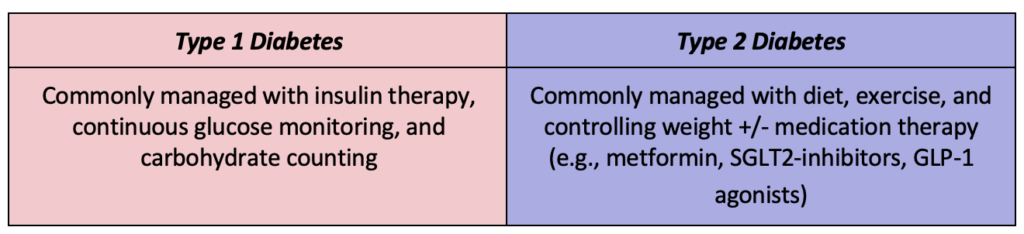
Management of Diabetes
There is a difference between how either condition is managed. Diet, exercise, drug therapy, and weight management (weight loss is more associated with T1DM whereas weight gain is more associated with T2DM) play critical roles in controlling blood sugar.
Understanding the difference between Type 1 and Type 2 diabetes is essential for effective management and improved health outcomes. Pharmacists as healthcare professionals can provide education, guidance, and support through helping individuals navigate the challenges of these conditions and work towards better health through a combination of lifestyle changes, medication management, and blood glucose monitoring.
Lin J, Thompson TJ, Cheng YJ, et al. Projection of the future diabetes burden in the United States through 2060. Population Health Metrics. 2018;16(1). doi:https://doi.org/10.1186/s12963-018-0166-4.
“Now remember to complete the entire course of your antibiotic until it’s finished, even if you feel better.”
How often has a patient heard this from either their doctor or pharmacist? Hopefully every time. As vital drugs, antibiotics have saved countless lives. Akin to other drugs, they can also be misused or overused. However, what sets them apart as a class of drugs is the unique threat that comes with their use: antibiotic resistance. Why is that a threat?
Understanding Antibiotic Resistance
Antibiotic resistance refers to the ability of microorganisms such as bacteria to continue to grow and ultimately defeat the very drug (antibiotic) intended to limit their growth or kill them altogether.1 In other words, the microorganism becomes resistant to the antibiotic treatment. Eventually, resistance of the microorganism to even one drug poses a risk to other drugs in the same class. When this occurs, infections become harder and harder to treat.
Now why this occurs is because bacteria can adapt and develop resistance through natural selection by the mere presence of antibiotics. The purpose of antibiotics is to kill bacteria, regardless of if they’re the bad bacteria that cause infection or the good bacteria that protect us from infection. Killing the good bacteria would cause loss of the protection that they normally provide allowing the bad bacteria to grow. What could make this worse?
Factors Contributing to Antibiotic Resistance
Incomplete courses of antibiotic treatment → by not finishing the entire course, bacteria that survived become resistant and multiply or pass on their resistant genes to other surviving bacteria
Inappropriate prescribing of an antibiotic → using an inappropriate antibiotic drug that wouldn’t effectively treat the infection or using antibiotics when not needed allows bacteria to spread and either worsen or cause an infection
Overprescribing of antibiotics → increased use of antibiotics gives bacteria more chances to grow, survive, and become resistant through multiple mechanisms of current and future antibiotics
The Consequences
If antibiotic resistance develops to the point of utilizing first-line treatment options, then use of second or third-line options may become necessary. However, they are not always ideal or as effective, and prolonged drug treatment use may cause serious side effects and may lead to a delay in recovery. In addition, some patients with chronic conditions may not have a strong immune system to fight off simple infections, much less infections from resistant bacteria. In addition, it is possible that in some cases there are not any more treatment options to continue. All these aspects contribute to increased healthcare costs, decreased effectiveness of interventions, and poor health outcomes for patients.
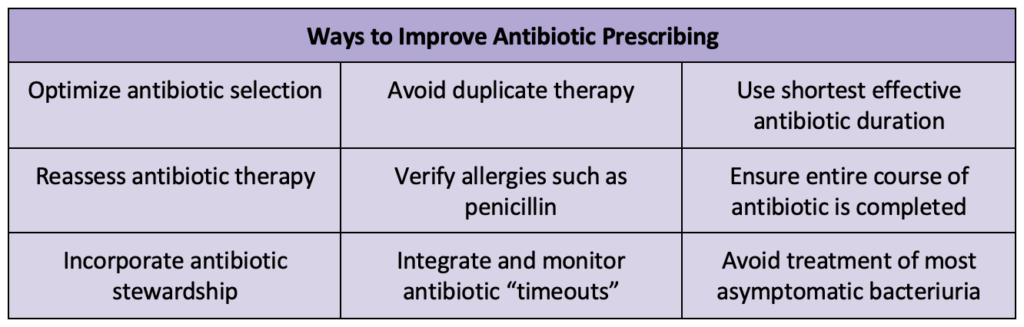
Pharmacists and Antibiotic Stewardship
Pharmacists play a vital role in promoting responsible, appropriate, and effective antibiotic use. Some interventions performed by pharmacists involve dose adjustments, dose optimization (increasing or decreasing the dose depending on patient’s health status), drug-interactions, stop orders that are time sensitive, changing IV antibiotics to oral formulation, and removing or discontinuing duplicate antibiotic therapy.3
Antibiotic resistance is a multifaceted challenge. Pharmacists have a vital role in educating patients, promoting responsible antibiotic use, and advocating for evidence-based prescribing practices. Their knowledge and skills allow them to provide education to both patients and other healthcare providers regarding adherence, drug dosing, and proper antibiotic use. Through collaboration with providers, proper and effective antibiotic use can improve and continue for all current and future generations.
In today’s world, pharmacists are no longer limited to the traditional role of dispensing prescriptions and have decided to make use of the ever-expanding potential of information technology. Pharmacy informatics continues to be a dynamic field, combining the impact of pharmacy with the force of technology to transform the way that pharmacists manage patient care, streamline operations, and improve health outcomes. Let’s delve a little bit more into this topic.
What is Pharmacy Informatics?
Pharmacy informatics is defined as the application of clinical knowledge and expertise in combination with the use of health information technology (HIT) to improve the processes of medication management and drug delivery.1 Pharmacists who work in this field, along with their knowledge and background in pharmacotherapy and pharmacy practice, have sufficient understanding of the discipline of informatics and health information technology.2
The Pharmacist’s Role
There are 5 basic responsibilities of pharmacists who work in pharmacy informatics.3 These have been defined by the American Society of Health-System Pharmacists (ASHP) as:
Information Management: overseeing medication management and sharing patient information to ensure patient safety
Bar code medication administration
Computerized provider order entry (CPOE)
Ease of information exchange among systems
Knowledge delivery: provision of knowledge and patient-specific information as clinical decision support
Clinical guidelines
Patient reports and summaries
Alerts and reminders
Optimizing electronic health records (EHR) to include mandatory indications and medication adjustments where appropriate
Data analytics: reviewing the data and analyzing it
Healthcare analytics- improving quality and efficiency of healthcare operations and processes by reviewing past performances
Clinical informatics: promoting the integration and application of information technology in healthcare settings for easier handoff and transition of care
Computerized medication reconciliation
Smart infusion pumps
Change management: the development, management, and continuous improvement of clinical information systems
Actively managing clinical decision support interventions to keep up with current and developing treatments
The Benefits and Challenges
Multiple advantages for adopting informatics exist in the form of reduced medication errors, improved medication adherence, and increased patient involvement. It is also important to highlight that decision making is being supported with data and facts to improve health outcomes for patients and contributes to evidence-based medicine (EBM) practices. As a result of using these systems and processes, pharmacists are able to identify potential drug-drug interactions, contraindications, and allergies with greater ease, safety, and efficiency.
That’s not to say that implementing pharmacy informatics systems comes without its challenges. One challenge lies in support training for all pharmacists so that there’s consistent quality of work and knowledge of using these systems across multiple settings. Another challenge includes maintaining proper safeguard measures and data security as more data is utilized in the healthcare setting. Some of these challenges can be overcome through continued education sessions, training and workshops, collaboration with IT for technology related developments, and staying open-minded to new technological innovations.
Closing Thoughts
Pharmacy informatics will continue to mold and reshape how pharmacy is being practiced. It has the ability to empower pharmacists in providing patient care that is safer and more efficient. Being more open-minded about the use of technology can open doors to embracing the optimization of medication management delivery so that the end result is improved patient health outcomes. Pharmacy informatics has the potential to change the future of healthcare and the future of pharmacy- let’s see where it will take us.